Pollari Francesco, Spadaccio Cristiano, Cuomo Michela, Chello Massimo, Nenna Antonio, Fischlein Theodor, Nappi Francesco
Department of Cardiac Surgery, Klinikum Nürnberg-Paracelsus Medical University, Nuremberg, Germany.
Department of Cardiac Surgery, Golden Jubilee National Hospital, Glasgow, UK.
Ann Transl Med. 2020 Dec;8(23):1624. doi: 10.21037/atm-20-4626.
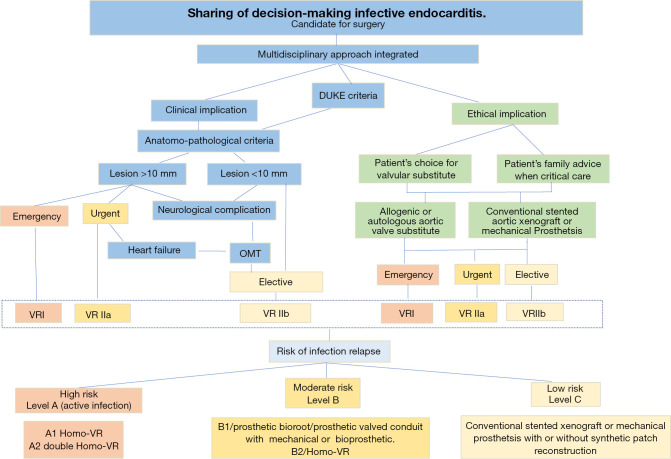
Infective endocarditis (IE) is nowadays one of the most challenging disease in cardiac surgery because of its multifaceted clinical and anatomical presentation. Despite the many clinical and surgical advances achieved in the past 60 years, there is a lack of evidence regarding the ideal strategy. The present review aims to investigate and highlight two main novel concepts for the decision-making of the best substitute. Firstly, the concept of an "endocarditis team": a coordinated multidisciplinary effort in the diagnostic work-up, especially in conditions of high risk of embolization or clinical deterioration. A good "endocarditis team" has the role to overcome such problem, in order to ensure a prompt and balanced strategy. Secondly, which ethical considerations are required to drive the choice of valvular substitute. The choice of best valve substitute is a relevant issue of debate, not only with operative but also prognostic and accordingly ethical aftermaths. Many different solutions have been developed to substitute the infected valve. Among these: mechanical prosthesis (MP), biological stented prosthesis (BP), sutureless bioprosthesis and cryopreserved homografts (CHs). Patients need to be informed in detail about the technical issues pertaining the use of these valve substitute. We will discuss the evidences regarding the risk of recurrent infections or future potentially severe calcification of aortic homograft valve and wall (in other words, the failure of the homograft) and the difficulties in managing the reoperation.
由于感染性心内膜炎(IE)具有多方面的临床和解剖学表现,如今它是心脏外科中最具挑战性的疾病之一。尽管在过去60年里取得了许多临床和外科进展,但关于理想策略仍缺乏证据。本综述旨在研究并强调两个主要的新概念,以用于最佳替代物决策。首先,“心内膜炎团队”的概念:在诊断检查中进行多学科协调努力,尤其是在栓塞风险高或临床病情恶化的情况下。一个优秀的“心内膜炎团队”应发挥作用克服此类问题,以确保采取及时且平衡的策略。其次,驱动瓣膜替代物选择需要考虑哪些伦理因素。最佳瓣膜替代物的选择是一个相关的争议问题,不仅涉及手术,还涉及预后以及相应的伦理后果。已经开发出许多不同的解决方案来替代感染的瓣膜。其中包括:机械假体(MP)、生物带支架假体(BP)、无缝合生物假体和冷冻保存同种异体移植物(CHs)。需要向患者详细告知与使用这些瓣膜替代物相关的技术问题。我们将讨论有关复发性感染风险或主动脉同种异体移植瓣膜及管壁未来潜在严重钙化(换句话说,同种异体移植物失败)的证据,以及再次手术管理中的困难。