Lavillegrand Jean-Rémi, Garnier Marc, Spaeth Agathe, Mario Nathalie, Hariri Geoffroy, Pilon Antoine, Berti Enora, Fieux Fabienne, Thietart Sara, Urbina Tomas, Turpin Matthieu, Darrivere Lucie, Fartoukh Muriel, Verdonk Franck, Dumas Guillaume, Tedgui Alain, Guidet Bertrand, Maury Eric, Chantran Yannick, Voiriot Guillaume, Ait-Oufella Hafid
Service de Médecine Intensive-Réanimation, Hôpital Saint-Antoine, Assistance Publique-Hôpitaux de Paris, 184 rue du faubourg Saint-Antoine, 75571, Paris cedex 12, France.
Sorbonne Université, Paris, France.
Ann Intensive Care. 2021 Jan 13;11(1):9. doi: 10.1186/s13613-020-00798-x.
SARS coronavirus 2 (SARS-CoV-2) is responsible for high morbidity and mortality worldwide, mostly due to the exacerbated inflammatory response observed in critically ill patients. However, little is known about the kinetics of the systemic immune response and its association with survival in SARS-CoV-2+ patients admitted in ICU. We aimed to compare the immuno-inflammatory features according to organ failure severity and in-ICU mortality.
Six-week multicentre study (N = 3) including SARS-CoV-2+ patients admitted in ICU. Analysis of plasma biomarkers at days 0 and 3-4 according to organ failure worsening (increase in SOFA score) and 60-day mortality.
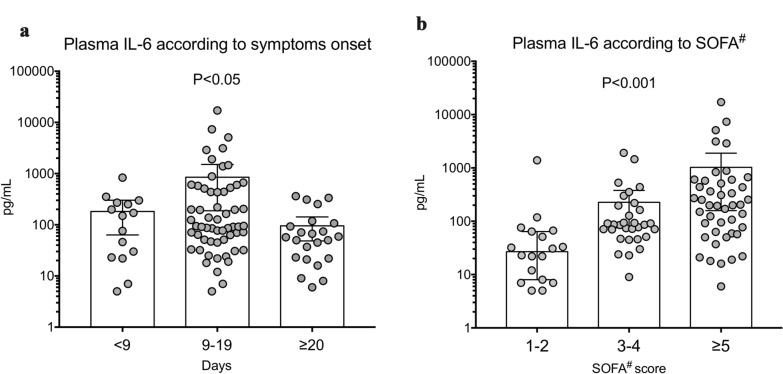
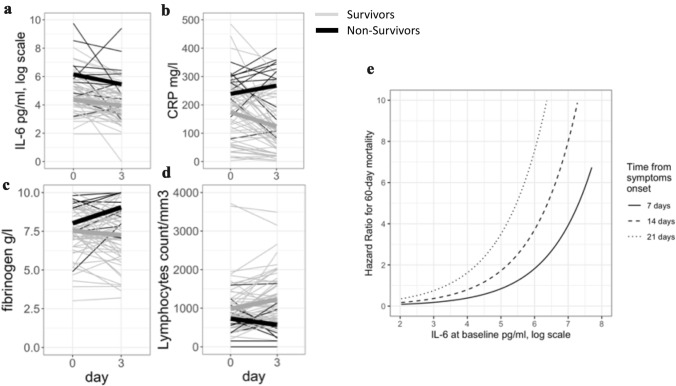
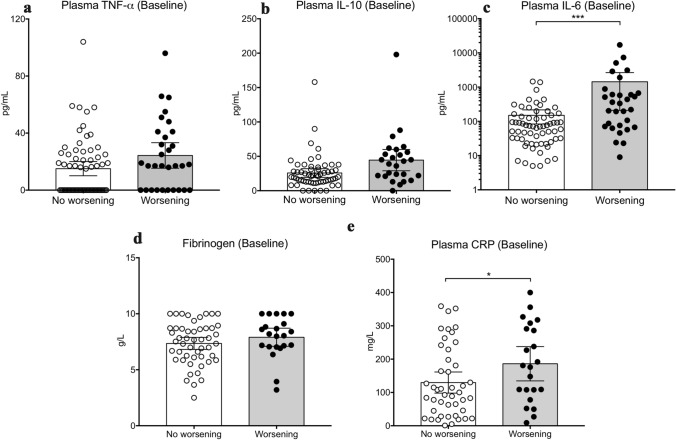
101 patients were included. Patients had severe respiratory diseases with PaO2/FiO2 of 155 [111-251] mmHg), SAPS II of 37 [31-45] and SOFA score of 4 [3-7]. Eighty-three patients (83%) required endotracheal intubation/mechanical ventilation and among them, 64% were treated with prone position. IL-1β was barely detectable. Baseline IL-6 levels positively correlated with organ failure severity. Baseline IL-6 and CRP levels were significantly higher in patients in the worsening group than in the non-worsening group (278 [70-622] vs. 71 [29-153] pg/mL, P < 0.01; and 178 [100-295] vs. 100 [37-213] mg/L, P < 0.05, respectively). Baseline IL-6 and CRP levels were significantly higher in non-survivors compared to survivors but fibrinogen levels and lymphocyte counts were not different between groups. After adjustment on SOFA score and time from symptom onset to first dosage, IL-6 and CRP remained significantly associated with mortality. IL-6 changes between Day 0 and Day 3-4 were not different according to the outcome. A contrario, kinetics of CRP and lymphocyte count were different between survivors and non-survivors.
In SARS-CoV-2+ patients admitted in ICU, a systemic pro-inflammatory signature was associated with clinical worsening and 60-day mortality.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)在全球范围内导致了高发病率和高死亡率,这主要归因于危重症患者中观察到的炎症反应加剧。然而,对于入住重症监护病房(ICU)的SARS-CoV-2阳性患者全身免疫反应的动力学及其与生存的关系知之甚少。我们旨在根据器官衰竭严重程度和ICU内死亡率比较免疫炎症特征。
一项为期六周的多中心研究(N = 3),纳入入住ICU的SARS-CoV-2阳性患者。根据器官衰竭恶化情况(序贯器官衰竭评估(SOFA)评分增加)和60天死亡率分析第0天和第3 - 4天的血浆生物标志物。
纳入101例患者。患者患有严重呼吸系统疾病,动脉血氧分压/吸入氧分数(PaO2/FiO2)为155[111 - 251]mmHg,简化急性生理学评分(SAPS)II为37[31 - 45],SOFA评分为4[3 - 7]。83例患者(83%)需要气管插管/机械通气,其中64%接受了俯卧位治疗。几乎检测不到白细胞介素-1β(IL-1β)。基线IL-6水平与器官衰竭严重程度呈正相关。恶化组患者的基线IL-6和C反应蛋白(CRP)水平显著高于未恶化组(分别为278[70 - 622]对71[29 - 153]pg/mL,P < 0.01;以及178[100 - 295]对100[37 - 213]mg/L,P < 0.05)。与幸存者相比,非幸存者的基线IL-6和CRP水平显著更高,但纤维蛋白原水平和淋巴细胞计数在两组之间没有差异。在对SOFA评分和从症状出现到首次给药的时间进行调整后,IL-6和CRP仍然与死亡率显著相关。根据预后情况,第0天和第3 - 4天之间IL-6的变化没有差异。相反,幸存者和非幸存者之间CRP和淋巴细胞计数的动力学不同。
在入住ICU的SARS-CoV-2阳性患者中,全身促炎特征与临床恶化和60天死亡率相关。