Clinical Epidemiology Division, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden.
Department of Surgery, Capio St Görans Hospital, Stockholm, Sweden.
JNCI Cancer Spectr. 2020 Sep 26;5(1). doi: 10.1093/jncics/pkaa084. eCollection 2021 Feb.
Although small, node-negative breast cancer (ie, T1abN0) constitutes 20% of all newly diagnosed breast cancers, data on prognosis and prognostic factors are limited.
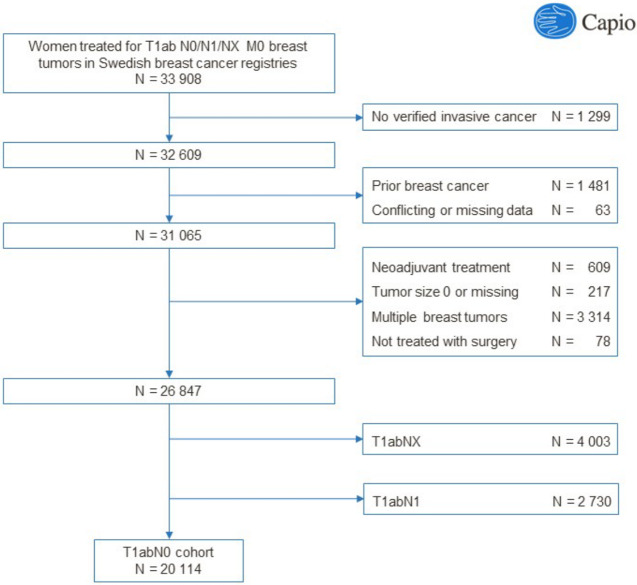
We conducted a population-based cohort study including 20 114 Swedish women treated for T1abN0 breast cancer from 1977 onward. Patient and tumor data were collected from Swedish breast cancer registries. Cohort subjects were followed through linkage to the Cause of Death Register. We calculated the cumulative incidence of breast cancer-specific and overall death and used Cox regression to estimate hazard ratios (HRs) and 95% confidence intervals (CIs).
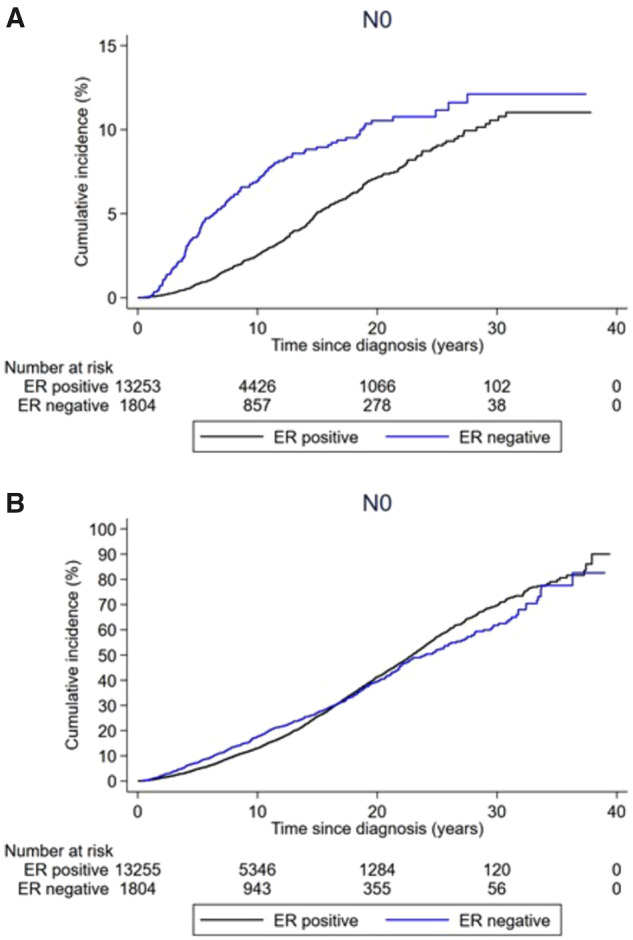
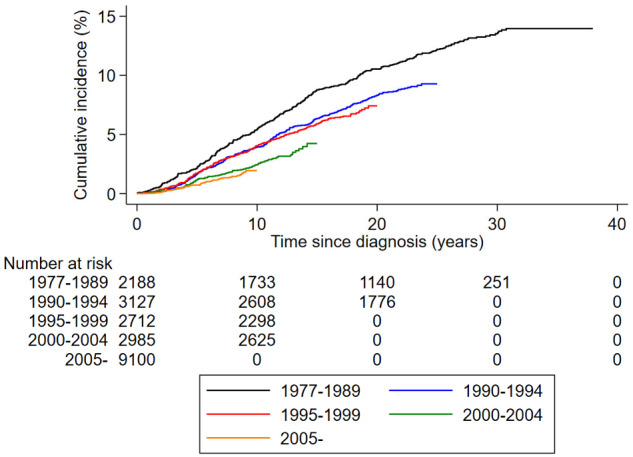
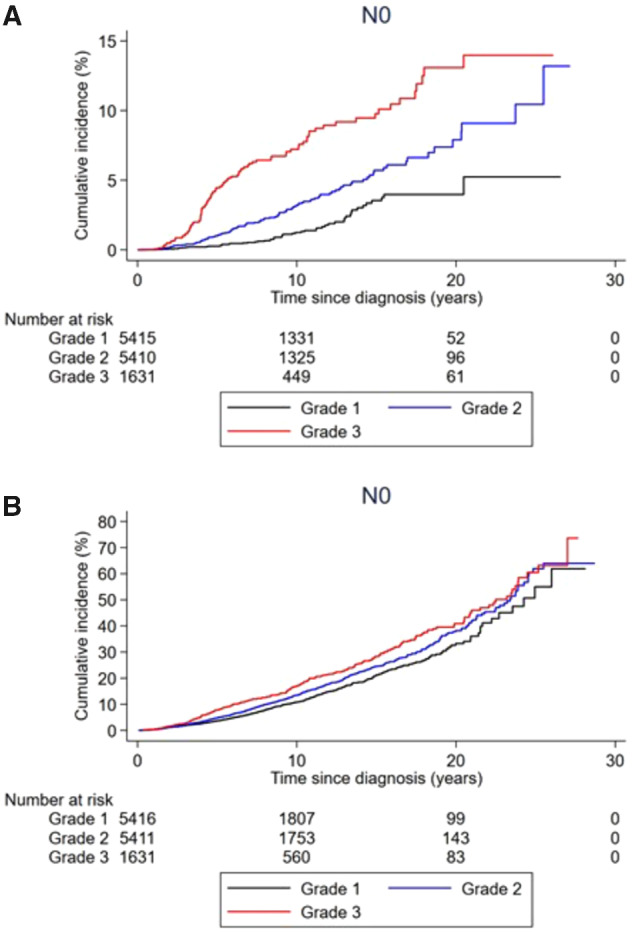
During a median follow-up of 9.1 years (range = 0-38), 915 women died of breast cancer and 5416 of any cause. The 10-, 20-, and 30-year cumulative incidences of breast cancer death were 3.4% (95% CI = 3.1% to 3.7%), 7.6% (95% CI = 7.1% to 8.2%), and 10.5% (95% CI = 9.6% to 11.4%), respectively. The multivariable hazard ratios and 95% confidence intervals of breast cancer death were 0.92 (95% CI = 0.88 to 0.97) for each additional calendar year of diagnosis, 4.38 (95% CI = 2.79 to 6.87) for grade 3 vs grade 1 tumors, 0.43 (95% CI = 0.31 to 0.62) for progesterone receptor-positive vs progesterone receptor-negative disease, and 2.01 (95% CI = 0.99 to 4.07) for HER2-positive vs HER2-negative disease. Women with grade 3 vs grade 1 tumors had a 56% increased risk of death from any cause (HR = 1.56, 95% CI = 1.30 to 1.88).
The risk of breast cancer death in T1abN0 disease continues to increase steadily beyond 10 years after diagnosis, has improved over time, and varies substantially by tumor characteristics.
虽然小,淋巴结阴性乳腺癌(即 T1abN0)构成了所有新诊断乳腺癌的 20%,但预后和预后因素的数据有限。
我们进行了一项基于人群的队列研究,纳入了 1977 年以来接受 T1abN0 乳腺癌治疗的 20114 名瑞典女性。患者和肿瘤数据来自瑞典乳腺癌登记处。队列受试者通过与死因登记处的链接进行随访。我们计算了乳腺癌特异性和总死亡的累积发生率,并使用 Cox 回归估计风险比(HR)和 95%置信区间(CI)。
在中位随访 9.1 年(范围=0-38)期间,915 名女性死于乳腺癌,5416 名女性死于其他任何原因。10 年、20 年和 30 年的乳腺癌死亡累积发生率分别为 3.4%(95%CI=3.1%至 3.7%)、7.6%(95%CI=7.1%至 8.2%)和 10.5%(95%CI=9.6%至 11.4%)。乳腺癌死亡的多变量风险比和 95%置信区间分别为每增加 1 年诊断时间为 0.92(95%CI=0.88 至 0.97)、3 级肿瘤与 1 级肿瘤相比为 4.38(95%CI=2.79 至 6.87)、孕激素受体阳性与孕激素受体阴性疾病相比为 0.43(95%CI=0.31 至 0.62)和 HER2 阳性与 HER2 阴性疾病相比为 2.01(95%CI=0.99 至 4.07)。3 级肿瘤患者的任何原因死亡风险增加 56%(HR=1.56,95%CI=1.30 至 1.88)。
T1abN0 疾病的乳腺癌死亡风险在诊断后 10 年以上持续稳步增加,且随时间推移而改善,且肿瘤特征差异显著。