Yan Shanshan, Wang Yongnan, Guo Yujuan, Zhang Yan, Peng Haiyan, Tang Huang, Luo Yizhong, Zhang Anqin, Gao Hongyi
Department of Pathology, Guangdong Women and Children Hospital, Guangzhou, Guangdong 511400, P.R. China.
Breast Disease Center, Guangdong Women and Children Hospital, Guangzhou, Guangdong 511400, P.R. China.
Oncol Lett. 2023 Sep 28;26(5):491. doi: 10.3892/ol.2023.14078. eCollection 2023 Nov.
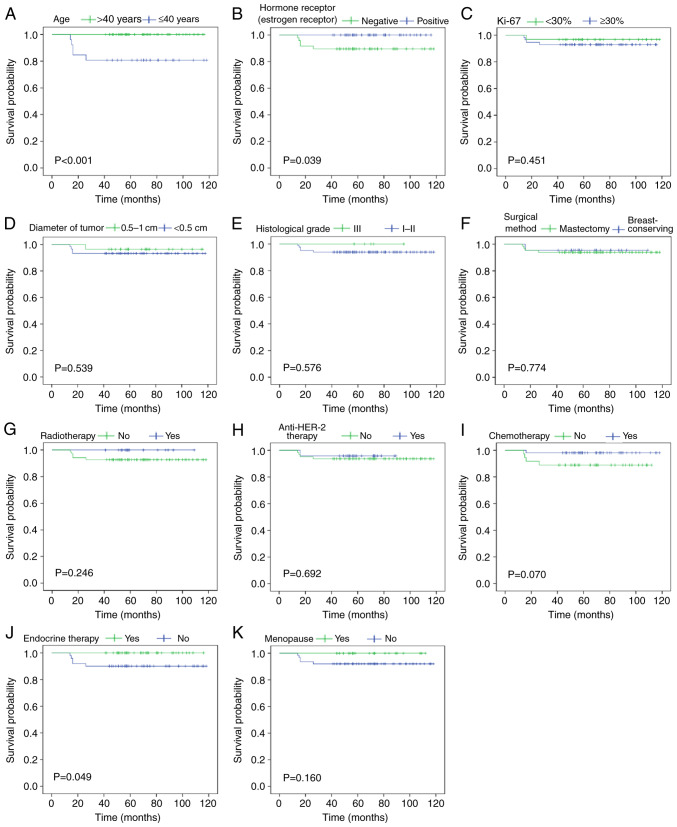
The 2021 National Comprehensive Cancer Network guidelines recommend that adjuvant chemotherapy combined with trastuzumab be considered for human epidermal growth factor receptor 2 (HER-2)-positive breast cancer patients with small tumors (tumor diameter ≤1 cm) and negative lymph nodes. Additionally, the prognostic factors and clinical significance of HER-2-positive breast cancer with negative lymph nodes and a tumor diameter ≤1 cm remain unclear. In the present study, the clinical data and prognostic factors of 87 patients with HER-2-positive breast cancer with negative lymph nodes and a tumor diameter ≤1 cm admitted to Guangdong Women and Children Hospital from January 2013 to December 2019 were retrospectively analyzed. The median follow-up time was 70 months, the disease-free survival (DFS) of all patients was 94.3% and the overall survival (OS) was 100%. Univariate analysis of prognosis demonstrated that patients aged ≤40 years had significantly lower DFS than those aged >40 (80.8 vs. 100.0%, P<0.001). DFS was significantly improved in patients who were hormone-receptor-positive and patients who received endocrine therapy compared with patients who were estrogen receptor negative and patients who did not receive endocrine therapy (100.0 vs. 89.6%, P=0.039; 100.0 vs. 90.0%, P=0.049). Prognostic univariate analysis demonstrated that patient age, hormone receptor status and use of endocrine therapy were significantly related to the DFS (P<0.05), while none of these were independent factors related to the DFS in the prognostic multivariate analysis (P=0.240, P=0.976 and P=0.925). The proportion of patients with a tumor diameter 0.5-1 cm receiving adjuvant anti-HER-2 treatment was significantly greater compared with patients with tumors with a diameter ≤0.5 cm (46.4 vs. 18.6%, P<0.05). There was no significance difference in the DFS of patients treated with adjuvant chemotherapy with or without anti-HER-2 therapy with tumor diameters ≤0.5 cm (P>0.05), but there was a significant difference in the DFS of patients with a tumor diameter 0.5-1 cm (P<0.05). These results suggested that adjuvant chemotherapy, with or without anti-HER-2 therapy, may affect the prognosis of HER-2-positive breast cancer patients with negative lymph nodes and a tumor diameter of 0.5-1 cm. Therefore, it could be recommended that such patients receive adjuvant chemotherapy and anti-HER-2 therapy in the future.
2021年美国国立综合癌症网络指南建议,对于肿瘤较小(肿瘤直径≤1 cm)且淋巴结阴性的人表皮生长因子受体2(HER-2)阳性乳腺癌患者,应考虑辅助化疗联合曲妥珠单抗治疗。此外,淋巴结阴性且肿瘤直径≤1 cm的HER-2阳性乳腺癌的预后因素及临床意义仍不明确。在本研究中,回顾性分析了2013年1月至2019年12月在广东省妇幼保健院收治的87例淋巴结阴性且肿瘤直径≤1 cm的HER-2阳性乳腺癌患者的临床资料及预后因素。中位随访时间为70个月,所有患者的无病生存率(DFS)为94.3%,总生存率(OS)为100%。预后的单因素分析显示,年龄≤40岁的患者DFS显著低于年龄>40岁的患者(80.8% vs. 100.0%,P<0.001)。与激素受体阴性且未接受内分泌治疗的患者相比,激素受体阳性且接受内分泌治疗的患者DFS显著改善(100.0% vs. 89.6%,P=0.039;100.0% vs. 90.0%,P=0.049)。预后单因素分析显示,患者年龄、激素受体状态及内分泌治疗的使用与DFS显著相关(P<0.05),而在预后多因素分析中这些均不是与DFS相关的独立因素(P=0.240、P=0.976及P=0.925)。肿瘤直径0.5-1 cm的患者接受辅助抗HER-2治疗的比例显著高于肿瘤直径≤0.5 cm的患者(46.4% vs. 18.6%,P<0.05)。肿瘤直径≤0.5 cm的患者接受或未接受抗HER-2治疗的辅助化疗,其DFS无显著差异(P>0.05),但肿瘤直径0.5-1 cm的患者DFS有显著差异(P<0.05)。这些结果提示,辅助化疗无论是否联合抗HER-2治疗,可能会影响淋巴结阴性且肿瘤直径为0.5-1 cm的HER-2阳性乳腺癌患者的预后。因此,建议未来此类患者接受辅助化疗及抗HER-2治疗。