Department of Clinical Pharmacy, Division of Laboratory Medicine and Pharmacy, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Center for Translational Immunology, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Br J Clin Pharmacol. 2021 Aug;87(8):3218-3226. doi: 10.1111/bcp.14738. Epub 2021 Feb 1.
Clofarabine has recently been evaluated as part of the conditioning regimen for allogeneic hematopoietic stem cell transplantation (HCT) in children. Pharmacokinetic (PK) exposure of different agents commonly used in conditioning regimens is strongly related to HCT outcome. Consequently, the PK of clofarabine may be important for outcome. This report describes the population PK of clofarabine in paediatric patients and one adult.
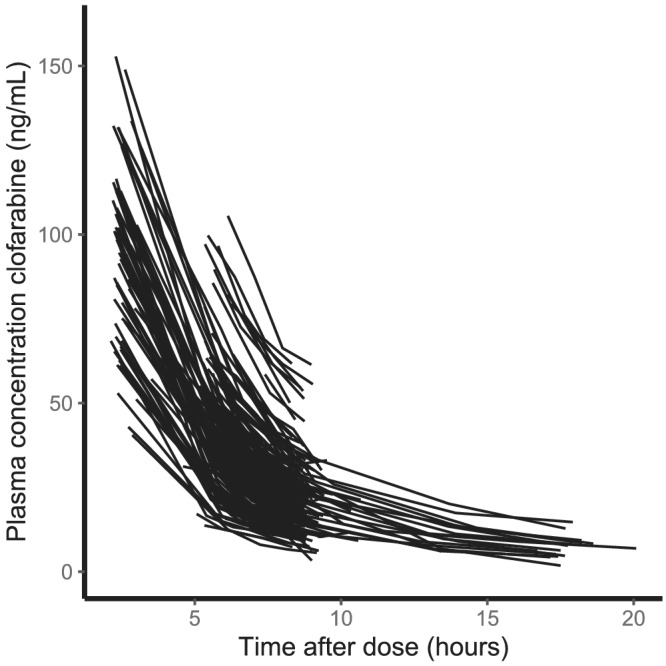
From 80 paediatric (0.5-18 years) and 1 adult patient (37 years), 805 plasma concentrations were included in pharmacokinetic analyses using nonlinear mixed effects modelling.
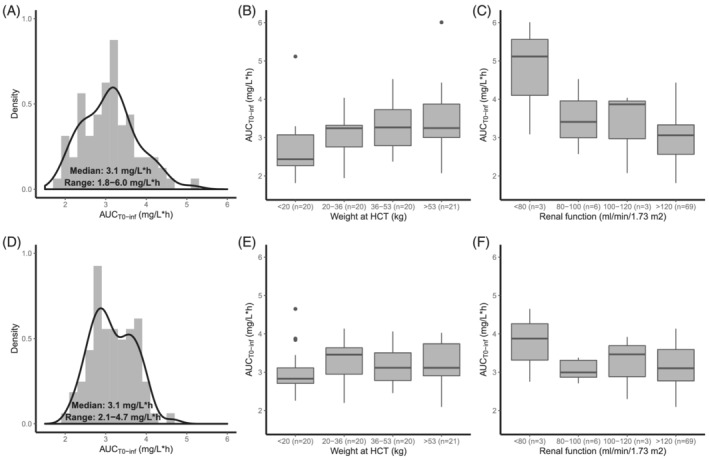
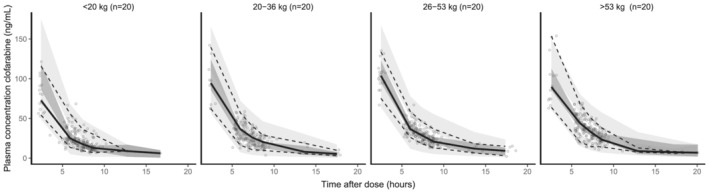
A two-compartment model adequately described the PK of clofarabine. Body weight and estimated glomerular filtration rate (eGFR) were included as covariates. Clearance was differentiated into nonrenal and renal clearance (approximately 55% of total clearance), resulting in population estimates of 24.0 L/h (95% confidence interval [CI] 13.7-34.4) and 29.8 L/h (95% CI 23.9-36.1) for a patient of 70 kg with normal renal function, respectively. Unexplained interindividual variability in clearance was 17.8% (95% CI 14.6-22.4). A high variability in exposure was observed (range area under the curve 1.8-6.0 mg/L*h) after body surface area (BSA) based dosing. Interestingly, children with low body weight had a lower exposure than children with a higher body weight, which indicates that the currently practised BSA-based dosing is not adequate for clofarabine.
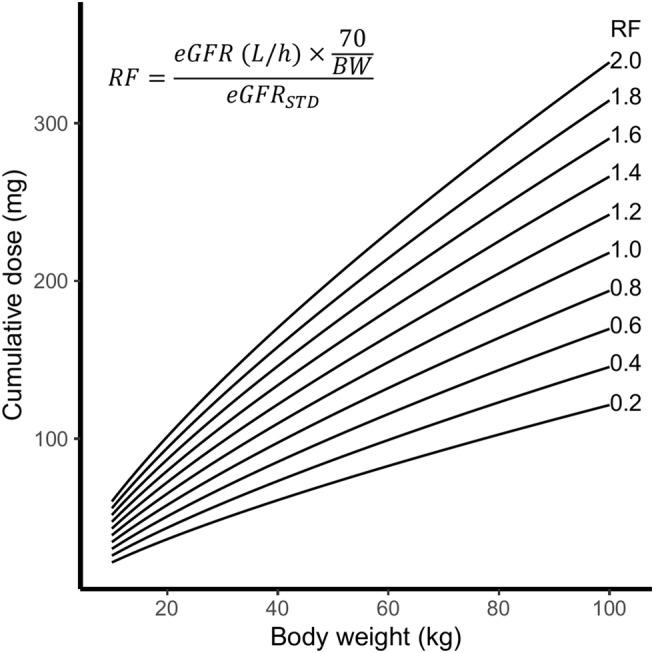
A clofarabine dosing algorithm based on this PK model, using body weight and eGFR, results in a more predictable exposure than BSA-based dosing. However, the exact target exposure needs to be further investigated.
克拉屈滨最近已被评估为异基因造血干细胞移植(HCT)中预处理方案的一部分。预处理方案中常用的不同药物的药代动力学(PK)暴露与 HCT 结果密切相关。因此,克拉屈滨的 PK 可能对结果很重要。本报告描述了儿科患者和 1 例成人患者中克拉屈滨的群体 PK。
从 80 例儿科(0.5-18 岁)和 1 例成人患者(37 岁)中,共纳入 805 个血浆浓度进行药代动力学分析,采用非线性混合效应模型。
克拉屈滨的 PK 可以用两室模型很好地描述。体重和估算肾小球滤过率(eGFR)被纳入协变量。清除率分为非肾清除率和肾清除率(约占总清除率的 55%),对于肾功能正常的 70kg 患者,分别得出人群估计值 24.0 L/h(95%置信区间[CI] 13.7-34.4)和 29.8 L/h(95% CI 23.9-36.1)。清除率的个体间差异无法解释,为 17.8%(95% CI 14.6-22.4)。暴露量的个体差异很大(范围 AUC 为 1.8-6.0mg/L*h),这表明基于体表面积(BSA)的剂量方案并不适合克拉屈滨。
基于该 PK 模型,使用体重和 eGFR 的克拉屈滨给药方案,与基于 BSA 的剂量方案相比,可获得更可预测的暴露量。然而,确切的目标暴露量需要进一步研究。