1st Department of Surgery and Interventional Gastroenterology, Semmelweis University, 1082 Üllői út 78, Budapest, Hungary.
Department of Anesthesiology and Intensive Therapy, Semmelweis University, 1082 Üllői út 78B, Budapest, Hungary.
BMC Anesthesiol. 2021 Jan 14;21(1):19. doi: 10.1186/s12871-021-01236-6.
Postoperative pulmonary complications (PPCs) are important contributors to mortality and morbidity after surgery. The available predicting models are useful in preoperative risk assessment, but there is a need for validated tools for the early postoperative period as well. Lung ultrasound is becoming popular in intensive and perioperative care and there is a growing interest to evaluate its role in the detection of postoperative pulmonary pathologies.
We aimed to identify characteristics with the potential of recognizing patients at risk by comparing the lung ultrasound scores (LUS) of patients with/without PPC in a 24-h postoperative timeframe.
Observational study at a university clinic. We recruited ASA 2-3 patients undergoing elective major abdominal surgery under general anaesthesia. LUS was assessed preoperatively, and also 1 and 24 h after surgery. Baseline and operative characteristics were also collected. A one-week follow up identified PPC+ and PPC- patients. Significantly differing LUS values underwent ROC analysis. A multi-variate logistic regression analysis with forward stepwise model building was performed to find independent predictors of PPCs.
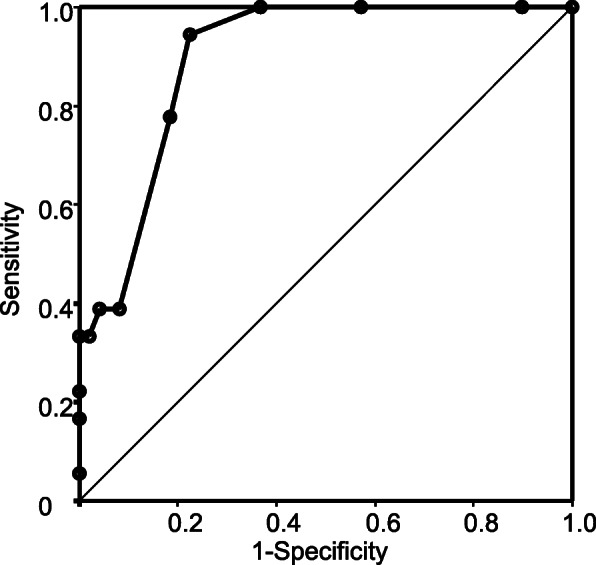
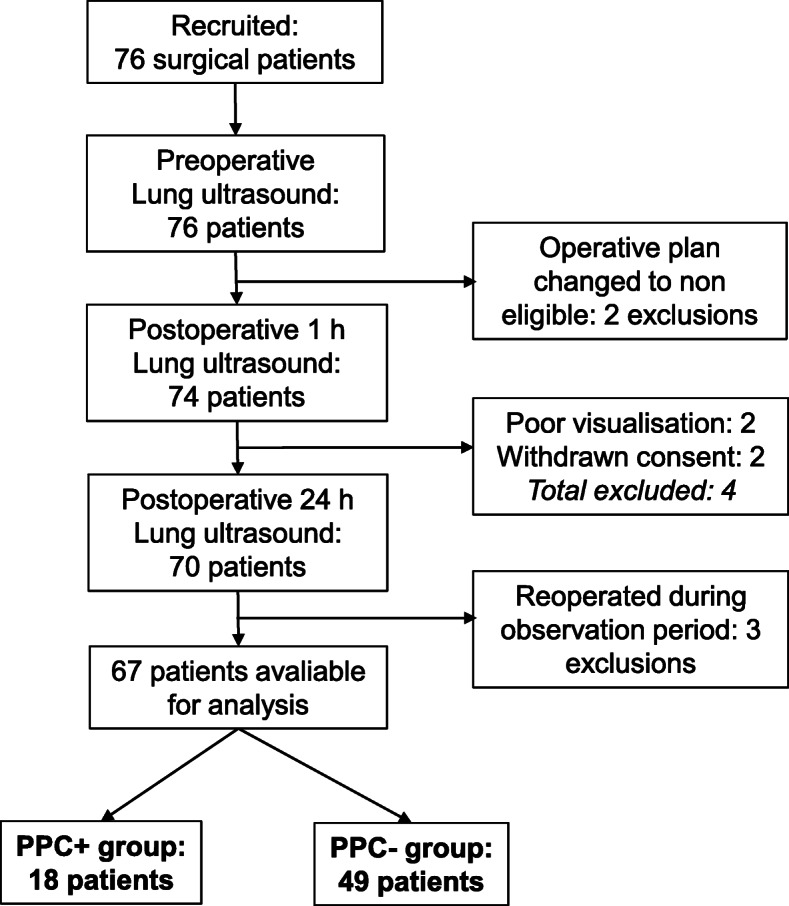
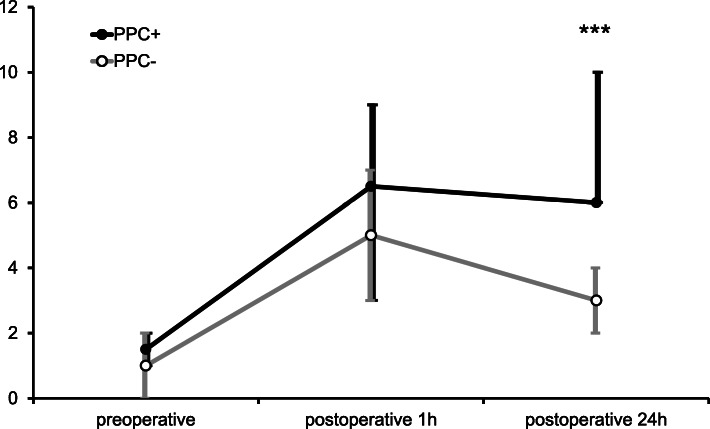
Out of the 77 recruited patients, 67 were included in the study. We evaluated 18 patients in the PPC+ and 49 in the PPC- group. Mean ages were 68.4 ± 10.2 and 66.4 ± 9.6 years, respectively (p = 0.4829). Patients conforming to ASA 3 class were significantly more represented in the PPC+ group (66.7 and 26.5%; p = 0.0026). LUS at baseline and in the postoperative hour were similar in both populations. The median LUS at 0 h was 1.5 (IQR 1-2) and 1 (IQR 0-2; p = 0.4625) in the PPC+ and PPC- groups, respectively. In the first postoperative hour, both groups had a marked increase, resulting in scores of 6.5 (IQR 3-9) and 5 (IQR 3-7; p = 0.1925). However, in the 24th hour, median LUS were significantly higher in the PPC+ group (6; IQR 6-10 vs 3; IQR 2-4; p < 0.0001) and it was an independent risk factor (OR = 2.6448 CI95% 1.5555-4.4971; p = 0.0003). ROC analysis identified the optimal cut-off at 5 points with high sensitivity (0.9444) and good specificity (0.7755).
Postoperative LUS at 24 h can identify patients at risk of or in an early phase of PPCs.
术后肺部并发症(PPCs)是手术后死亡和发病的重要原因。现有的预测模型在术前风险评估中很有用,但也需要验证工具来评估术后早期的情况。肺部超声在重症监护和围手术期护理中越来越受欢迎,人们对其在检测术后肺部病变方面的作用也越来越感兴趣。
我们旨在通过比较术后 24 小时内 PPC 患者和非 PPC 患者的肺部超声评分(LUS),确定有潜在风险的患者的特征。
这是在一所大学诊所进行的观察性研究。我们招募了 ASA 2-3 级、接受全身麻醉下择期大腹部手术的患者。术前、术后 1 小时和 24 小时评估 LUS,并收集基线和手术特征。一周的随访确定 PPC+和 PPC-患者。对差异有统计学意义的 LUS 值进行 ROC 分析。采用逐步向前法建立多元逻辑回归分析,寻找 PPC 的独立预测因素。
在 77 名入选患者中,有 67 名患者入组。我们评估了 18 名 PPC+患者和 49 名 PPC-患者。平均年龄分别为 68.4±10.2 岁和 66.4±9.6 岁(p=0.4829)。ASA 3 级患者在 PPC+组中更为常见(66.7%和 26.5%;p=0.0026)。两组患者的基线和术后 LUS 相似。PPC+组和 PPC-组 0 小时时的中位数 LUS 分别为 1.5(IQR 1-2)和 1(IQR 0-2;p=0.4625)。在术后第一小时,两组 LUS 均明显升高,分别为 6.5(IQR 3-9)和 5(IQR 3-7;p=0.1925)。然而,在 24 小时时,PPC+组的中位数 LUS 明显更高(6;IQR 6-10 与 3;IQR 2-4;p<0.0001),且是独立的危险因素(OR=2.6448,95%CI95% 1.5555-4.4971;p=0.0003)。ROC 分析确定 5 分作为最佳截断值,具有较高的敏感性(0.9444)和良好的特异性(0.7755)。
术后 24 小时的 LUS 可识别有 PPC 风险或处于早期阶段的患者。