Medical Oncology Department, University Hospital A Coruña, Xubias de Arriba, 84, 15006, A Coruña, Galicia, Spain.
Complexo Hospitalario Universitario de Ourense, Ourense, Galicia, Spain.
BMC Cancer. 2021 Jan 14;21(1):64. doi: 10.1186/s12885-020-07758-5.
Outcomes are poorer in metastatic colorectal cancer (mCRC) patients with BRAF V600E mutations than those without it, but the effect of these mutations on treatment response is unclear. This real-world study assessed the effects of antiangiogenic-based treatment and systemic inflammatory factors on outcomes in patients with BRAF V600-mutated mCRC.
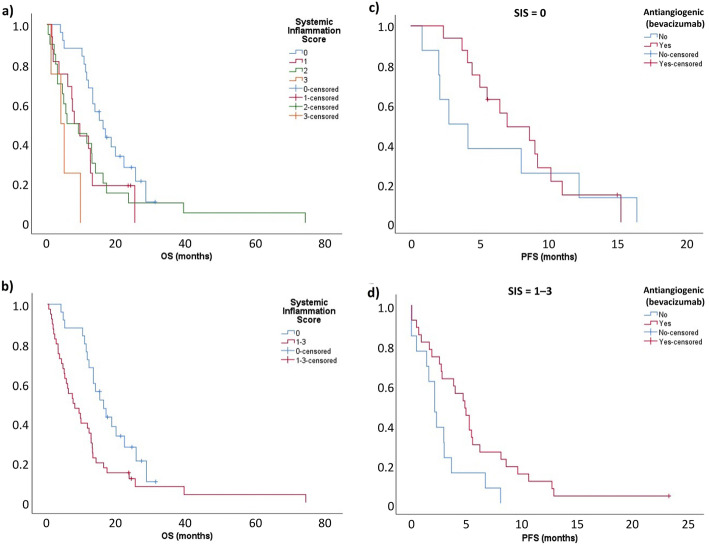
This real-world, multicenter, retrospective, observational study included patients with BRAF V600-mutated mCRC treated in eight hospitals in Spain. The primary endpoints were overall survival (OS) and progression-free survival (PFS); overall response rate (ORR) and disease control rate (DCR) were also assessed. The effect of first- and second-line treatment type on OS, PFS, ORR, and DCR were evaluated, plus the impact of systemic inflammatory markers on these outcomes. A systemic inflammation score (SIS) of 1-3 was assigned based on one point each for platelet-lymphocyte ratio (PLR) ≥200, neutrophil-lymphocyte ratio (NLR) ≥3, and serum albumin < 3.6 g/dL.
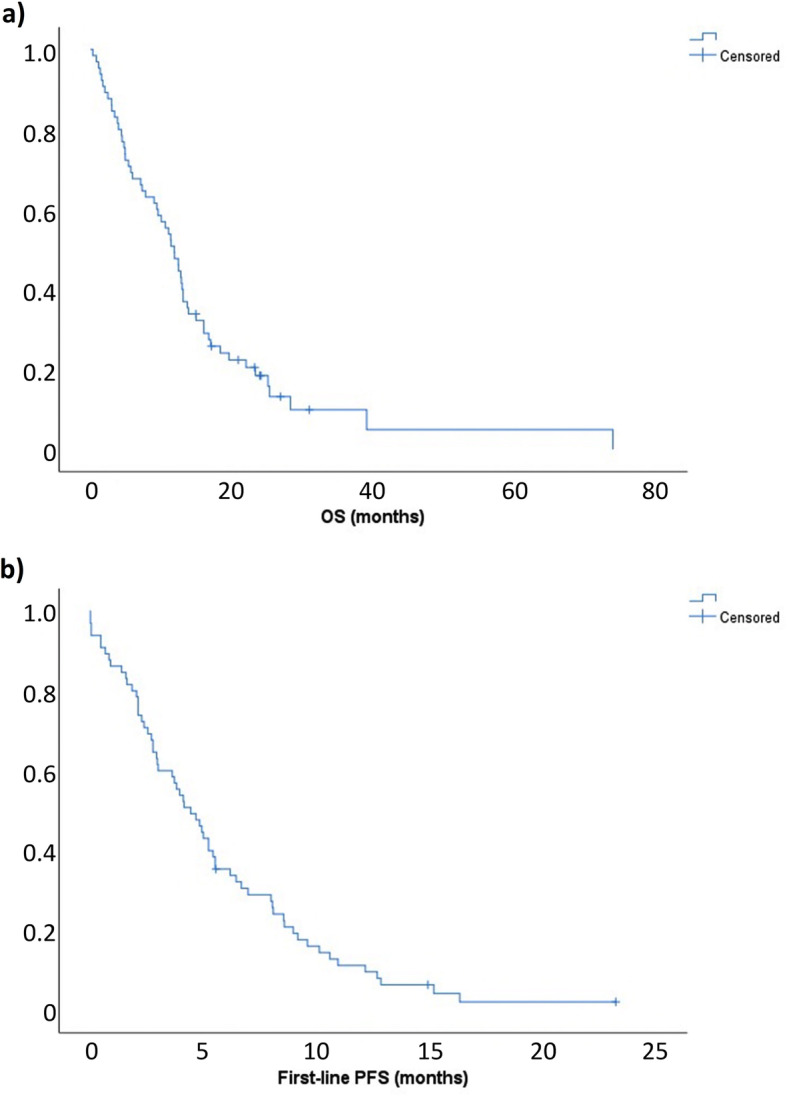
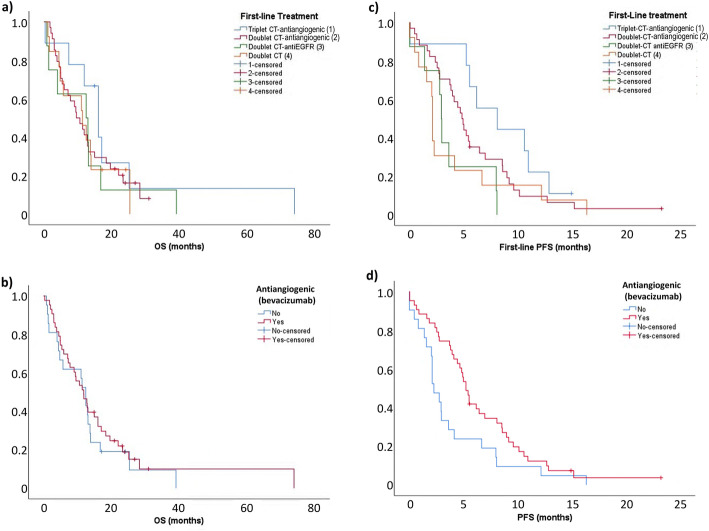
Of 72 patients, data from 64 were analyzed. After a median of 69.1 months, median OS was 11.9 months and median first-line PFS was 4.4 months. First-line treatment was triplet chemotherapy-antiangiogenic (12.5%), doublet chemotherapy-antiangiogenic (47.2%), doublet chemotherapy-anti-EGFR (11.1%), or doublet chemotherapy (18.1%). Although first-line treatment showed no significant effect on OS, antiangiogenic-based regimens were associated with prolonged median PFS versus non-antiangiogenic regimens. Negative predictors of survival with antiangiogenic-based treatment were NLR, serum albumin, and SIS 1-3, but not PLR. Patients with SIS 1-3 showed significantly prolonged PFS with antiangiogenic-based treatment versus non-antiangiogenic-based treatment, while those with SIS=0 showed no PFS benefit.
Antiangiogenic-based regimens, SIS, NLR, and albumin were predictors of survival in patients with mCRC, while SIS, NLR and serum albumin may predict response to antiangiogenic-based chemotherapy.
GIT-BRAF-2017-01.
BRAF V600E 突变的转移性结直肠癌(mCRC)患者的预后比没有突变的患者差,但这些突变对治疗反应的影响尚不清楚。这项真实世界的研究评估了抗血管生成治疗和全身炎症因子对 BRAF V600 突变 mCRC 患者结局的影响。
这是一项真实世界、多中心、回顾性、观察性研究,纳入了在西班牙 8 家医院接受治疗的 BRAF V600 突变的 mCRC 患者。主要终点为总生存期(OS)和无进展生存期(PFS);还评估了总缓解率(ORR)和疾病控制率(DCR)。评估了一线和二线治疗类型对 OS、PFS、ORR 和 DCR 的影响,以及全身炎症标志物对这些结局的影响。根据血小板-淋巴细胞比值(PLR)≥200、中性粒细胞-淋巴细胞比值(NLR)≥3 和血清白蛋白<3.6g/dL,分别计 1 分,确定了一个全身炎症评分(SIS)为 1-3。
在 72 名患者中,有 64 名患者的数据进行了分析。中位随访 69.1 个月后,中位 OS 为 11.9 个月,中位一线 PFS 为 4.4 个月。一线治疗为三联化疗-抗血管生成(12.5%)、双药化疗-抗血管生成(47.2%)、双药化疗-抗 EGFR(11.1%)或双药化疗(18.1%)。尽管一线治疗对 OS 无显著影响,但抗血管生成方案与非抗血管生成方案相比,中位 PFS 延长。抗血管生成治疗的生存不良预测因素为 NLR、血清白蛋白和 SIS 1-3,但不是 PLR。SIS 1-3 的患者接受抗血管生成治疗的 PFS 明显延长,而非 SIS 1-3 的患者则无 PFS 获益。
抗血管生成方案、SIS、NLR 和白蛋白是 mCRC 患者生存的预测因素,而 SIS、NLR 和血清白蛋白可能预测抗血管生成化疗的反应。
GIT-BRAF-2017-01。