Bayomy Ahmad F, Schickendantz Mark S, Briskin Isaac N, Farrow Lutul D, Grobaty Lauren E, Jones Morgan H, McCoy Brett W, Miniaci Anthony, Ricchetti Eric T, Rosneck James T, Sosic Elizabeth, Spindler Kurt P, Stearns Kim L, Strnad Greg J, Williams James, Saluan Paul M
Investigation performed at the Cleveland Clinic, Cleveland, Ohio, USA.
Orthop J Sports Med. 2020 Dec 29;8(12):2325967120966343. doi: 10.1177/2325967120966343. eCollection 2020 Dec.
Prospectively collected responses to Patient Acceptable Symptom State (PASS) questions after shoulder instability surgery are limited. Responses to these outcome measures are imperative to understanding their clinical utility.
PURPOSE/HYPOTHESIS: The purpose of this study was to evaluate which factors predict unfavorable patient-reported outcomes after shoulder instability surgery, including "no" to the PASS question. We hypothesized that poor outcomes would be associated with male adolescents, bone loss, combined labral tears, and articular cartilage injuries.
Cohort study; Level of evidence, 2.
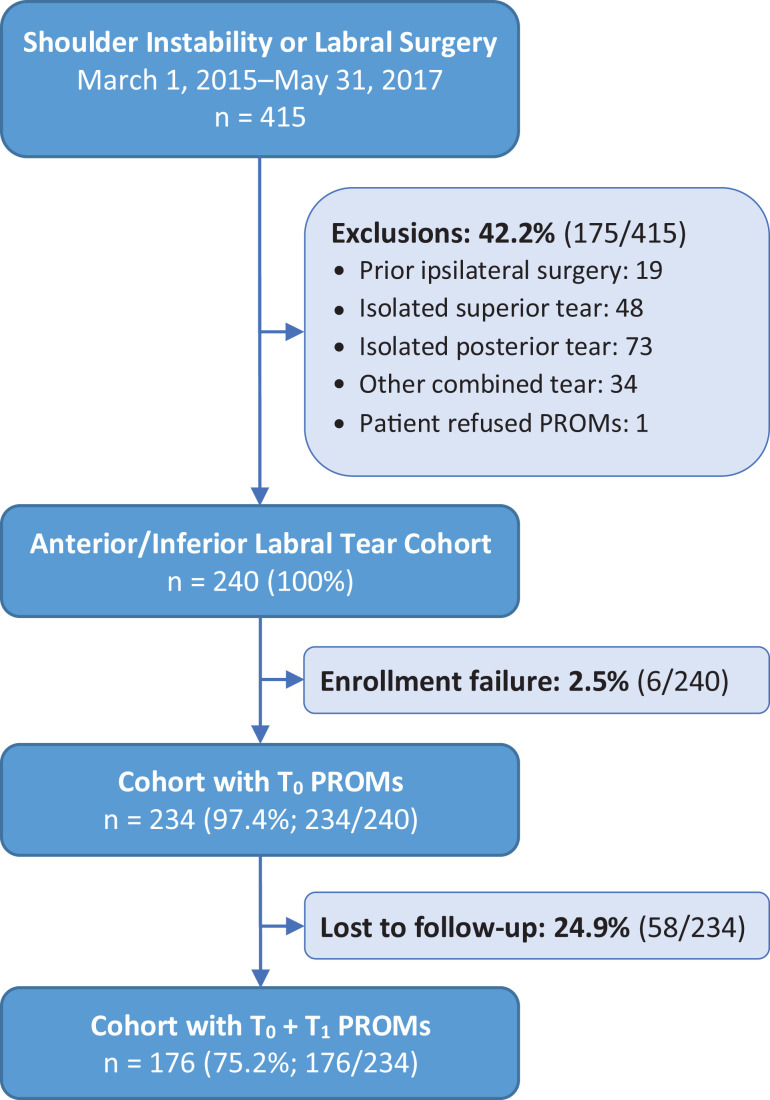
Patients aged ≥13 years undergoing shoulder instability surgery were included in point-of-care data collection at a single institution across 12 surgeons between 2015 and 2017. Patients with anterior-inferior labral tears were included, and those with previous ipsilateral shoulder surgery were excluded. Demographics, American Shoulder and Elbow Surgeons (ASES) and Single Assessment Numeric Evaluation (SANE) scores, and surgical findings were obtained at baseline. ASES and SANE scores, PASS responses, and early revision surgery rates were obtained at a minimum of 1 year after the surgical intervention. Regression analyses were performed.
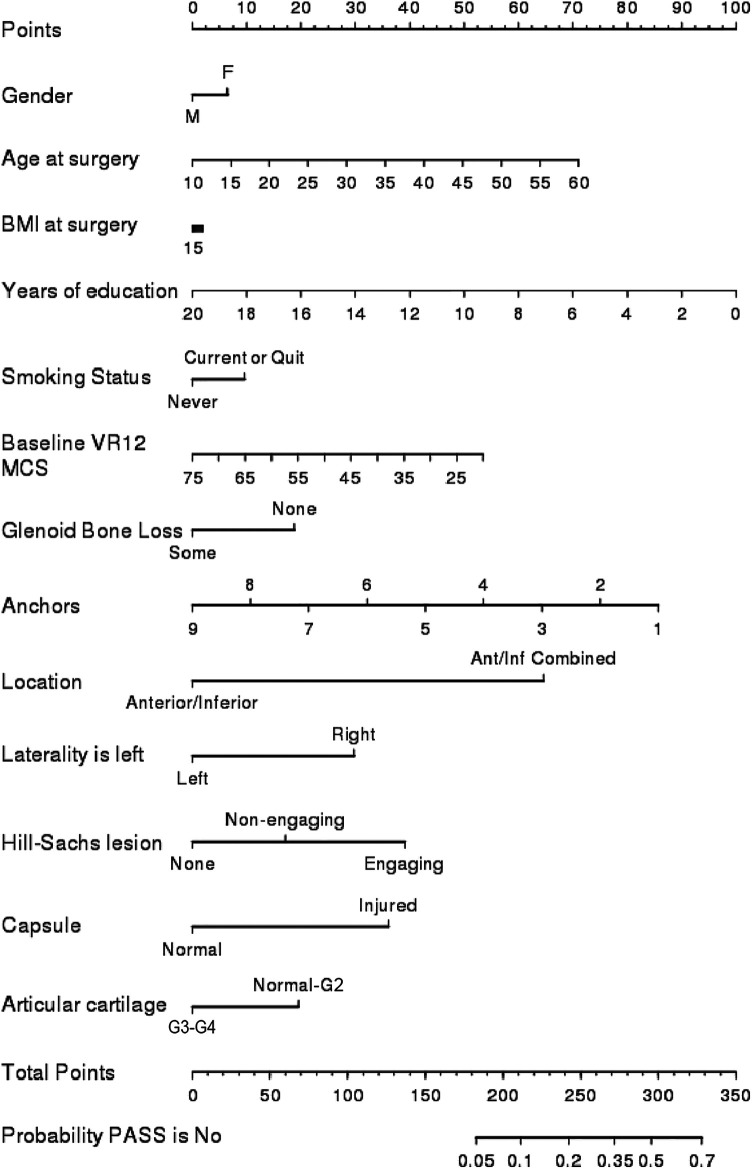
A total of 234 patients met inclusion criteria, of which 176 completed follow-up responses (75.2%). Nonresponders had a younger age, greater frequency of glenoid bone loss, fewer combined tears, and more articular cartilage injuries ( < .05). Responders' mean age was 25.1 years, and 22.2% were female. Early revision surgery occurred in 3.4% of these patients, and 76.1% responded yes to the PASS question. A yes response correlated with a mean 25-point improvement in the ASES score and a 40-point improvement in the SANE score. On multivariate analysis, combined labral tears (anterior-inferior plus superior or posterior tears) were associated with greater odds of responding no to the PASS question, while both combined tears and injured capsules were associated with lower ASES and SANE scores ( < .05). Sex, bone loss, and grade 3 to 4 articular cartilage injuries were not associated with variations on any patient-reported outcome measure.
Patients largely approved of their symptom state at ≥1 year after shoulder instability surgery. A response of yes to the PASS question was given by 76.1% of patients and was correlated with clinically and statistically significant improvements in ASES and SANE scores. Combined labral tears and injured capsules were negative prognosticators across patient-reported outcome measures, whereas sex, bone loss, and cartilage injuries were not.
前瞻性收集的肩部不稳定手术后患者对可接受症状状态(PASS)问题的回答有限。了解这些结局指标的临床效用,对这些指标的回答至关重要。
目的/假设:本研究的目的是评估哪些因素可预测肩部不稳定手术后患者报告的不良结局,包括对PASS问题回答“否”。我们假设不良结局与男性青少年、骨质流失、合并盂唇撕裂和关节软骨损伤有关。
队列研究;证据等级,2级。
纳入2015年至2017年期间在一家机构接受肩部不稳定手术且年龄≥13岁的患者,由12位外科医生进行即时医疗数据收集。纳入伴有前下盂唇撕裂的患者,排除既往同侧肩部手术患者。在基线时获取人口统计学资料、美国肩肘外科医师学会(ASES)和单评估数值评定(SANE)评分以及手术结果。在手术干预后至少1年时获取ASES和SANE评分、PASS回答以及早期翻修手术率。进行回归分析。
共有234例患者符合纳入标准;其中176例完成随访回答(75.2%)。未回答者年龄较小,肩胛盂骨质流失频率更高,合并撕裂较少,关节软骨损伤更多(P<0.05)。回答者的平均年龄为25.1岁,女性占22.2%。这些患者中有3.4%接受了早期翻修手术,76.1%对PASS问题回答“是”。回答“是”与ASES评分平均提高25分和SANE评分提高40分相关。多因素分析显示,合并盂唇撕裂(前下加上方或后方撕裂)与对PASS问题回答“否”的可能性更大有关,而合并撕裂和关节囊损伤均与较低的ASES和SANE评分相关(P<0.05)。性别、骨质流失和3至4级关节软骨损伤与任何患者报告的结局指标变化均无关。
肩部不稳定手术后≥1年时,患者对其症状状态大多表示认可。76.1%的患者对PASS问题回答“是”,这与ASES和SANE评分在临床和统计学上的显著改善相关。合并盂唇撕裂和关节囊损伤是患者报告结局指标的不良预后因素,而性别、骨质流失和软骨损伤则不是。