Malignant Hematology Department, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL.
Sidney Kimmel Comprehensive Cancer Center, Johns Hopkins University, Baltimore, MD.
J Clin Oncol. 2021 May 10;39(14):1584-1594. doi: 10.1200/JCO.20.02341. Epub 2021 Jan 15.
Approximately 20% of patients with -mutant myelodysplastic syndromes (MDS) achieve complete remission (CR) with hypomethylating agents. Eprenetapopt (APR-246) is a novel, first-in-class, small molecule that restores wild-type p53 functions in -mutant cells.
This was a phase Ib/II study to determine the safety, recommended phase II dose, and efficacy of eprenetapopt administered in combination with azacitidine in patients with -mutant MDS or acute myeloid leukemia (AML) with 20%-30% marrow blasts (ClinicalTrials.gov identifier: NCT03072043).
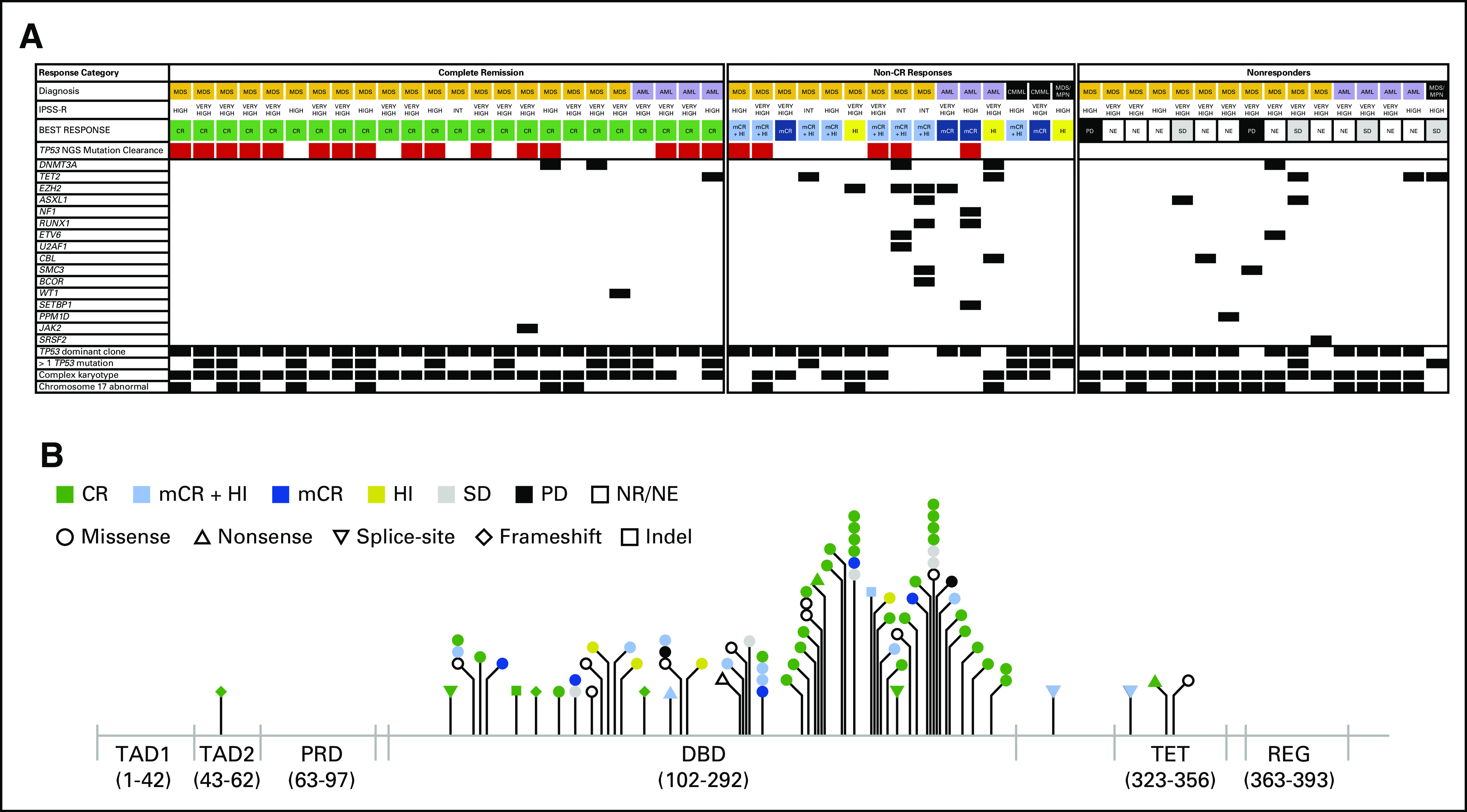
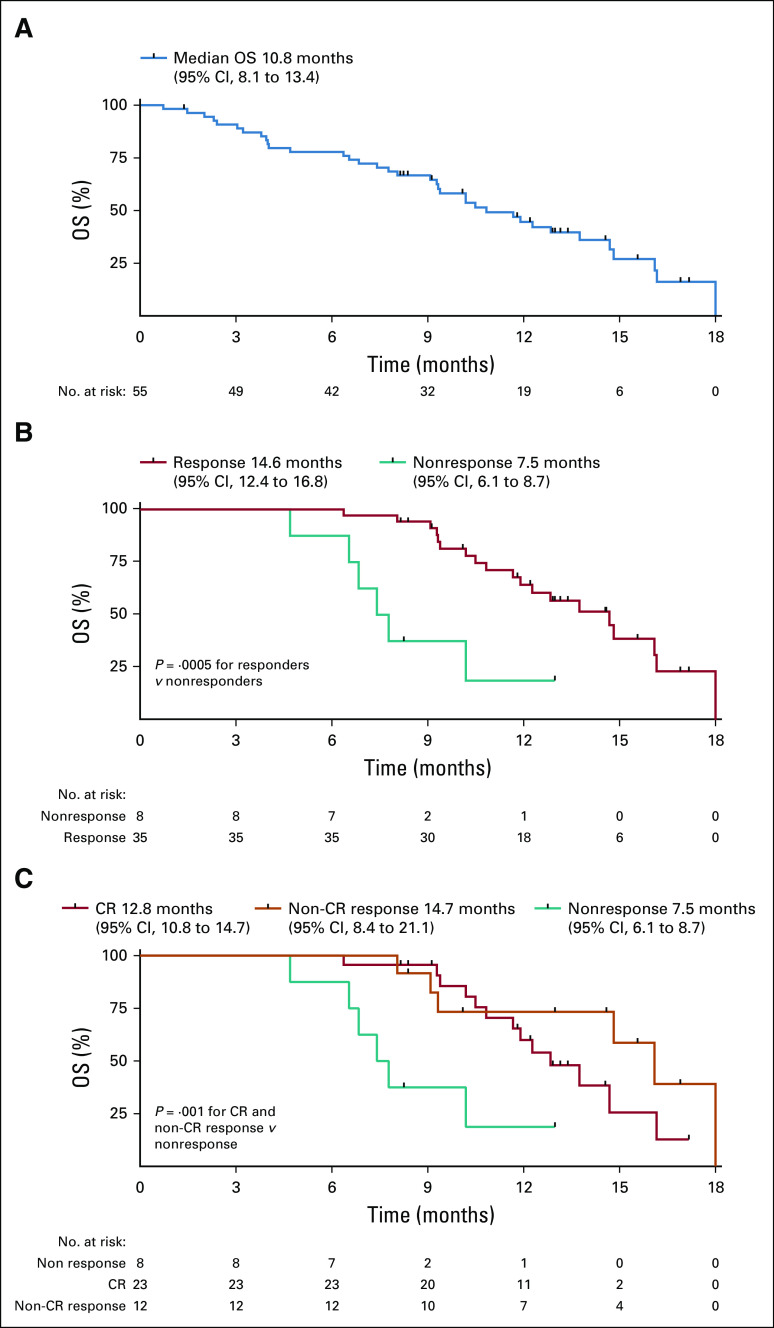
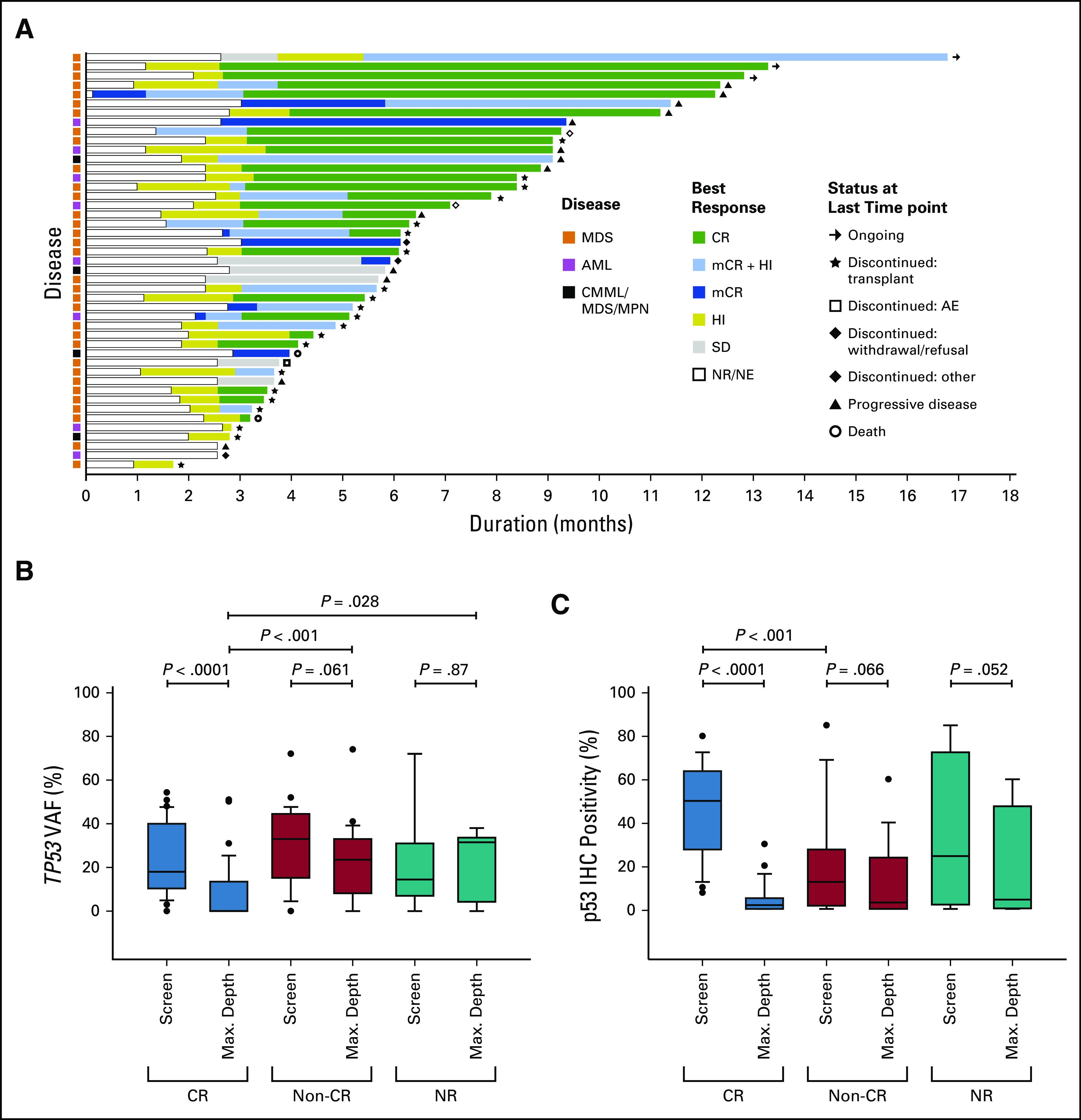
Fifty-five patients (40 MDS, 11 AML, and four MDS/myeloproliferative neoplasms) with at least one mutation were treated. The overall response rate was 71% with 44% achieving CR. Of patients with MDS, 73% (n = 29) responded with 50% (n = 20) achieving CR and 58% (23/40) a cytogenetic response. The overall response rate and CR rate for patients with AML was 64% (n = 7) and 36% (n = 4), respectively. Patients with only mutations by next-generation sequencing had higher rates of CR (69% 25%; = .006). Responding patients had significant reductions in variant allele frequency and p53 expression by immunohistochemistry, with 21 (38%) achieving complete molecular remission (variant allele frequency < 5%). Median overall survival was 10.8 months with significant improvement in responding versus nonresponding patients by landmark analysis (14.6 7.5 months; = .0005). Overall, 19/55 (35%) patients underwent allogeneic hematopoietic stem-cell transplant, with a median overall survival of 14.7 months. Adverse events were similar to those reported for azacitidine or eprenetapopt monotherapy, with the most common grade ≥ 3 adverse events being febrile neutropenia (33%), leukopenia (29%), and neutropenia (29%).
Combination treatment with eprenetapopt and azacitidine is well-tolerated yielding high rates of clinical response and molecular remissions in patients with -mutant MDS and oligoblastic AML.
大约 20%的 -突变型骨髓增生异常综合征(MDS)患者使用低甲基化药物可达到完全缓解(CR)。Eprenetapopt(APR-246)是一种新型的、首创的、小分子药物,可恢复 -突变细胞中的野生型 p53 功能。
这是一项 I/II 期研究,旨在确定 Eprenetapopt 联合阿扎胞苷在 -突变型 MDS 或伴有 20%-30%骨髓原始细胞的急性髓系白血病(AML)患者中的安全性、推荐的 II 期剂量和疗效(ClinicalTrials.gov 标识符:NCT03072043)。
55 例至少有一种 突变的患者(40 例 MDS、11 例 AML 和 4 例 MDS/骨髓增生性肿瘤)接受了治疗。总体缓解率为 71%,其中 44%达到 CR。在 MDS 患者中,73%(29 例)有反应,其中 50%(20 例)达到 CR,58%(23/40)有细胞遗传学反应。AML 患者的总体缓解率和 CR 率分别为 64%(7 例)和 36%(4 例)。通过下一代测序仅检测到 突变的患者 CR 率更高(69%,25%; =.006)。有反应的患者通过免疫组化检测到 等位基因频率和 p53 表达显著降低,其中 21 例(38%)达到完全分子缓解( 等位基因频率 < 5%)。中位总生存期为 10.8 个月,通过 landmark 分析,有反应的患者与无反应的患者相比有显著改善(14.6 7.5 个月; =.0005)。总体而言,55 例患者中有 19 例(35%)接受了同种异体造血干细胞移植,中位总生存期为 14.7 个月。不良事件与阿扎胞苷或 Eprenetapopt 单药治疗报告的不良事件相似,最常见的 3 级以上不良事件为发热性中性粒细胞减少症(33%)、白细胞减少症(29%)和中性粒细胞减少症(29%)。
Eprenetapopt 联合阿扎胞苷的联合治疗耐受性良好,在 -突变型 MDS 和少突细胞性 AML 患者中可获得较高的临床缓解率和分子缓解率。