Department of Leukemia, Unit 428, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX, 77030, USA.
Department of Biostatistics, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
J Hematol Oncol. 2023 Jul 8;16(1):73. doi: 10.1186/s13045-023-01476-8.
Pevonedistat is a first-in-class, small molecular inhibitor of NEDD8-activating enzyme that has clinical activity in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS). Preclinical data suggest synergy of pevonedistat with azacitidine and venetoclax.
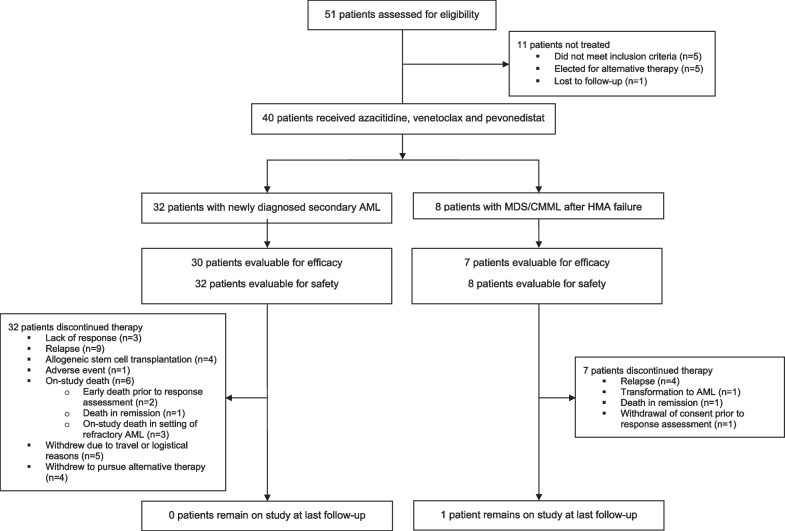
This single-center, phase 1/2 study evaluated the combination of azacitidine, venetoclax and pevonedistat in older adults with newly diagnosed secondary AML or with MDS or chronic myelomonocytic leukemia (CMML) after failure of hypomethylating agents. Patients received azacitidine 75 mg/m IV on days 1-7, venetoclax at maximum dose of 200-400 mg orally on days 1-21 (AML cohort) or days 1-14 (MDS/CMML cohort) and pevonedistat 20 mg/m IV on days 1, 3 and 5 for up to 24 cycles. The primary endpoints for the phase 2 portion of the study were the CR/CRi rate in the AML cohort and the overall response rate (CR + mCR + PR + HI) in the MDS/CMML cohort.
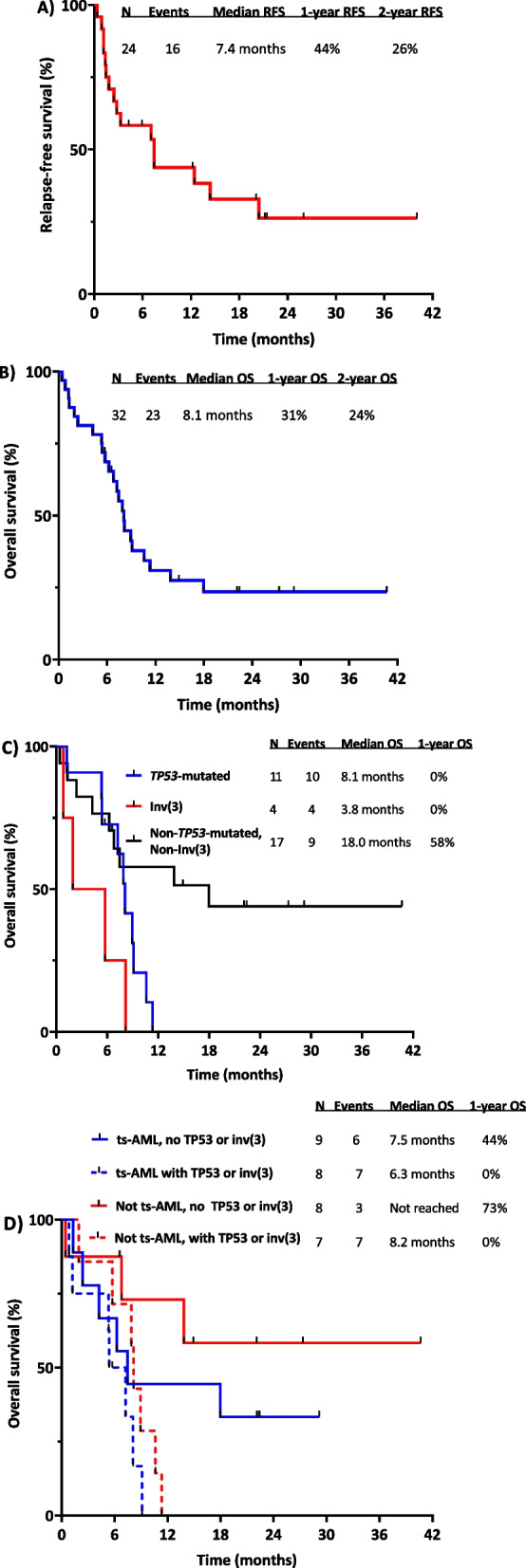
Forty patients were enrolled (32 with AML and 8 with MDS/CMML). In the AML cohort, the median age was 74 years (range 61-86 years), and 27 patients (84%) had at least one adverse risk cyto-molecular feature, including 15 (47%) with a TP53 mutation or MECOM rearrangement; seventeen patients (53%) had received prior therapy for a preceding myeloid disorder. The CR/CRi rate was 66% (CR 50%; CRi 16%), and the median overall survival (OS) was 8.1 months. In the MDS/CMML cohort, 7 patients (87%) were high or very high risk by the IPSS-R. The overall response rate was 75% (CR 13%; mCR with or without HI 50%; HI 13%). The most common grade 3-4 adverse events were infection in 16 patients (35%), febrile neutropenia in 10 patients (25%) and hypophosphatemia in 9 patients (23%). In an exploratory analysis, early upregulation of NOXA expression was observed, with subsequent decrease in MCL-1 and FLIP, findings consistent with preclinical mechanistic studies of pevonedistat. Upregulation of CD36 was observed, which may have contributed to therapeutic resistance.
The triplet combination of azacitidine, venetoclax and pevonedistat shows encouraging activity in this very poor-risk population of patients with AML, MDS or CMML. Trial registration ClinicalTrials.gov (NCT03862157).
Pevonedistat 是一种首创的小分子 NEDD8 激活酶抑制剂,在急性髓系白血病(AML)和骨髓增生异常综合征(MDS)中具有临床活性。临床前数据表明 Pevonedistat 与阿扎胞苷和 Venetoclax 具有协同作用。
这项单中心、1 期/2 期研究评估了阿扎胞苷、Venetoclax 和 Pevonedistat 联合治疗新诊断的继发性 AML 或接受低甲基化药物治疗失败后的 MDS 或慢性粒单核细胞白血病(CMML)患者。患者接受阿扎胞苷 75mg/m2,静脉滴注,第 1-7 天;Venetoclax 最大剂量 200-400mg,口服,第 1-21 天(AML 队列)或第 1-14 天(MDS/CMML 队列);Pevonedistat 20mg/m2,静脉滴注,第 1、3 和 5 天,最多 24 个周期。该研究 2 期部分的主要终点是 AML 队列的完全缓解/完全缓解伴血细胞计数不完全恢复(CR/CRi)率和 MDS/CMML 队列的总缓解率(CR+微小反应+部分反应+非常好的部分反应)。
共纳入 40 例患者(AML 32 例,MDS/CMML 8 例)。AML 队列的中位年龄为 74 岁(61-86 岁),27 例(84%)至少有一种不良风险细胞分子特征,包括 15 例(47%)有 TP53 突变或 MECOM 重排;17 例(53%)患者曾接受过治疗髓系疾病的先前治疗。CR/CRi 率为 66%(CR 50%;CRi 16%),中位总生存期(OS)为 8.1 个月。在 MDS/CMML 队列中,7 例患者(87%)根据 IPSS-R 为高危或极高危。总缓解率为 75%(CR 13%;mCR 伴或不伴 HI 50%;HI 13%)。最常见的 3-4 级不良事件是 16 例(35%)感染、10 例(25%)发热性中性粒细胞减少和 9 例(23%)低磷血症。在一项探索性分析中,观察到 NOXA 表达的早期上调,随后 MCL-1 和 FLIP 减少,这与 Pevonedistat 的临床前机制研究结果一致。观察到 CD36 的上调,这可能导致治疗耐药。
阿扎胞苷、Venetoclax 和 Pevonedistat 的三联疗法在 AML、MDS 或 CMML 这些高危患者人群中显示出令人鼓舞的活性。临床试验注册:ClinicalTrials.gov(NCT03862157)。