Boeke Caroline E, Joseph Jessica, Atem Charles, Banda Clement, Coulibaly Khady Diatou, Doi Naoko, Gunda Andrews, Kandulu James, Kiernan Brianán, Kingwara Leonard, Maokola Werner, Maparo Tatenda, Mbaye Rose Nadege, Mtumbuka Esther, Mziray Joseph, Ngugi Catherine, Nkakulu Jeanine, Nzuobontane Divine, Okomo Assoumo Marie Claire, Peter Trevor, Rioja Maria R, Sacks Jilian A, Simbi Raiva, Vojnov Lara, Khan Shaukat A
Clinton Health Access Initiative, Boston, MA, USA.
Clinton Health Access Initiative, Yaounde, Cameroon.
J Int AIDS Soc. 2021 Jan;24(1):e25663. doi: 10.1002/jia2.25663.
In many low- and middle-income countries, HIV viral load (VL) testing occurs at centralized laboratories and time-to-result-delivery is lengthy, preventing timely monitoring of HIV treatment adherence. Near point-of-care (POC) devices, which are placed within health facility laboratories rather than clinics themselves (i.e. "true" POC), can offer VL in conjunction with centralized laboratories to expedite clinical decision making and improve outcomes, especially for patients at high risk of treatment failure. We assessed impacts of near-POC VL testing on result receipt and clinical action in public sector programmes in Cameroon, Democratic Republic of Congo, Kenya, Malawi, Senegal, Tanzania and Zimbabwe.
Routine health data were collected retrospectively after introducing near-POC VL testing at 57 public sector health facilities (2017 to 2019, country-dependent). Where possible, key indicators were compared to data from patients receiving centralized laboratory testing using hazard ratios and the Somers' D test.
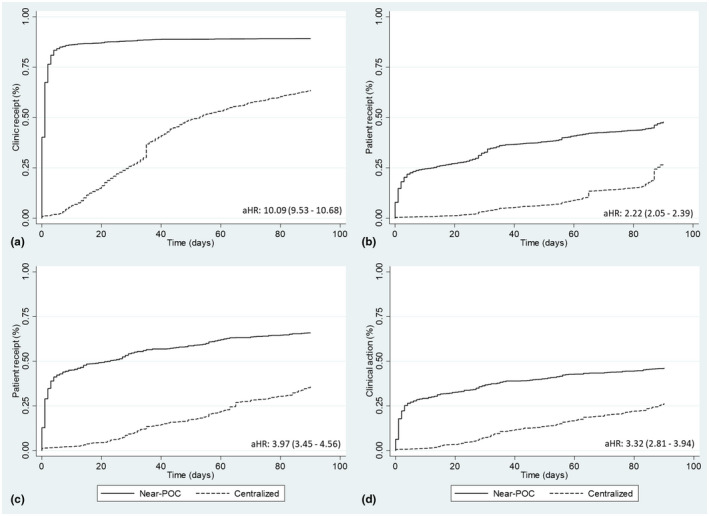
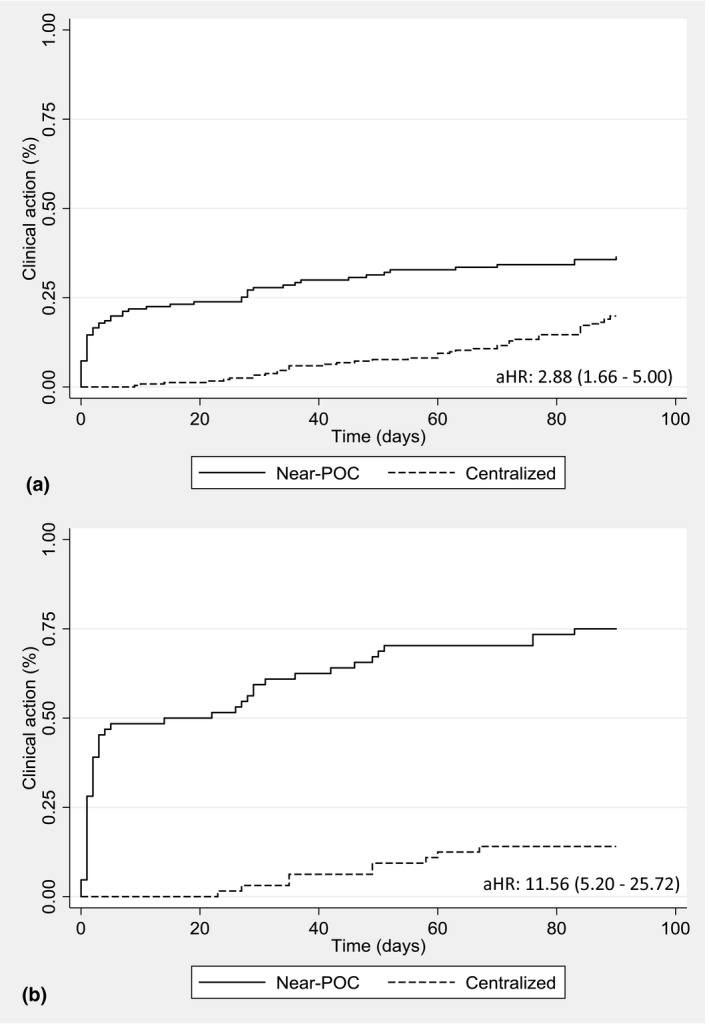
Data were collected from 6795 tests conducted on near-POC and 17614 tests on centralized laboratory-based platforms. Thirty-one percent (2062/6694) of near-POC tests were conducted for high-risk populations: pregnant and breastfeeding women, children and those with suspected failure. Compared to conventional testing, near-POC improved the median time from sample collection to return of results to patient [six vs. sixty-eight days, effect size: -32.2%; 95% CI: -41.0% to -23.4%] and to clinical action for individuals with an elevated HIV VL [three vs. fourty-nine days, effect size: -35.4%; 95% CI: -46.0% to -24.8%]. Near-POC VL results were two times more likely to be returned to the patient within 90 days compared to centralized tests [50% (1781/3594) vs. 27% (4172/15271); aHR: 2.22, 95% CI: 2.05 to 2.39]. Thirty-seven percent (340/925) of patients with an elevated near-POC HIV VL result had documented clinical follow-up actions within 30 days compared to 7% (167/2276) for centralized testing.
Near-POC VL testing enabled rapid test result delivery for high-risk populations and led to significant improvements in the timeliness of patient result receipt compared to centralized testing. While there was some improvement in time-to-clinical action with near-POC VL testing, major gaps remained. Strengthening of systems supporting the utilization of results for patient management are needed to truly capitalize on the benefits of decentralized testing.
在许多低收入和中等收入国家,HIV病毒载量(VL)检测在集中实验室进行,结果反馈时间较长,阻碍了对HIV治疗依从性的及时监测。近床旁(POC)设备放置在医疗机构实验室而非诊所本身(即“真正的”POC),可与集中实验室联合提供病毒载量检测,以加快临床决策并改善治疗效果,特别是对于有治疗失败高风险的患者。我们评估了近床旁病毒载量检测对喀麦隆、刚果民主共和国、肯尼亚、马拉维、塞内加尔、坦桑尼亚和津巴布韦公共部门项目中结果接收和临床行动的影响。
在57个公共部门医疗机构引入近床旁病毒载量检测后(2017年至2019年,因国家而异),回顾性收集常规健康数据。在可能的情况下,使用风险比和索莫斯D检验将关键指标与接受集中实验室检测的患者数据进行比较。
收集了6795次近床旁检测和17614次基于集中实验室平台检测的数据。31%(2062/6694)的近床旁检测针对高风险人群:孕妇和哺乳期妇女、儿童以及疑似治疗失败的患者。与传统检测相比,近床旁检测缩短了从样本采集到向患者反馈结果的中位时间[6天对68天,效应大小:-32.2%;95%CI:-41.0%至-23.4%],以及HIV病毒载量升高个体的临床行动时间[3天对49天,效应大小:-35.4%;95%CI:-46.0%至-24.8%]。与集中检测相比,近床旁病毒载量检测结果在90天内反馈给患者的可能性高出两倍[50%(1781/3594)对27%(4172/15271);aHR:2.22,95%CI:2.05至2.39]。近床旁HIV病毒载量检测结果升高的患者中,37%(340/925)在30天内有记录的临床随访行动,而集中检测为7%(167/2276)。
近床旁病毒载量检测能够为高风险人群快速提供检测结果,与集中检测相比,显著提高了患者接收结果的及时性。虽然近床旁病毒载量检测在临床行动时间上有一定改善,但仍存在重大差距。需要加强支持将检测结果用于患者管理的系统,以真正利用分散检测的益处。