Saito Suzue, Duong Yen T, Metz Melissa, Lee Kiwon, Patel Hetal, Sleeman Katrina, Manjengwa Julius, Ogollah Francis M, Kasongo Webster, Mitchell Rick, Mugurungi Owen, Chimbwandira Frank, Moyo Crispin, Maliwa Vusumuzi, Mtengo Helecks, Nkumbula Tepa, Ndongmo Clement B, Vere Nora Skutayi, Chipungu Geoffrey, Parekh Bharat S, Justman Jessica, Voetsch Andrew C
ICAP at Columbia University, New York, NY, USA.
Department of Epidemiology, Mailman School of Public Health at Columbia University, New York, NY, USA.
J Int AIDS Soc. 2017 Nov;20 Suppl 7(Suppl 7). doi: 10.1002/jia2.25004.
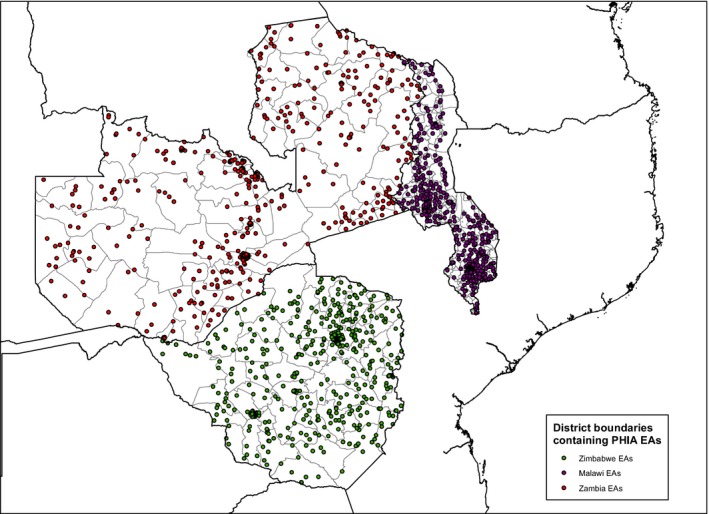
Logistical complexities of returning laboratory test results to participants have precluded most population-based HIV surveys conducted in sub-Saharan Africa from doing so. For HIV positive participants, this presents a missed opportunity for engagement into clinical care and improvement in health outcomes. The Population-based HIV Impact Assessment (PHIA) surveys, which measure HIV incidence and the prevalence of viral load (VL) suppression in selected African countries, are returning VL results to health facilities specified by each HIV positive participant within eight weeks of collection. We describe the performance of the specimen and data management systems used to return VL results to PHIA participants in Zimbabwe, Malawi and Zambia.
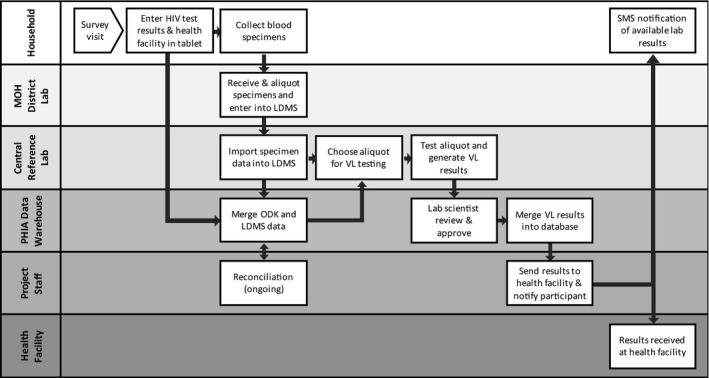
Consenting participants underwent home-based counseling and HIV rapid testing as per national testing guidelines; all confirmed HIV positive participants had VL measured at a central laboratory on either the Roche CAP/CTM or Abbott m2000 platform. On a bi-weekly basis, a dedicated data management team produced logs linking the VL test result with the participants' contact information and preferred health facility; project staff sent test results confidentially via project drivers, national courier systems, or electronically through an adapted short message service (SMS). Participants who provided cell phone numbers received SMS or phone call alerts regarding availability of VL results.
From 29,634 households across the three countries, 78,090 total participants 0 to 64 years in Zimbabwe and Malawi and 0 to 59 years in Zambia underwent blood draw and HIV testing. Of the 8391 total HIV positive participants identified, 8313 (99%) had VL tests performed and 8245 (99%) of these were returned to the selected health facilities. Of the 5979 VL results returned in Zimbabwe and Zambia, 85% were returned within the eight-week goal with a median turnaround time of 48 days (IQR: 33 to 61). In Malawi, where exact return dates were unavailable all 2266 returnable results reached the health facilities by 11 weeks.
The first three PHIA surveys returned the vast majority of VL results to each HIV positive participant's preferred health facility within the eight-week target. Even in the absence of national VL monitoring systems, a system to return VL results from a population-based survey is feasible, but it requires developing laboratory and data management systems and dedicated staff. These are likely important requirements to strengthen return of results systems in routine clinical care.
将实验室检测结果反馈给参与者存在后勤方面的复杂性,这使得撒哈拉以南非洲地区开展的大多数基于人群的艾滋病毒调查无法做到这一点。对于艾滋病毒呈阳性的参与者而言,这意味着失去了参与临床护理并改善健康结果的机会。基于人群的艾滋病毒影响评估(PHIA)调查旨在测量选定非洲国家的艾滋病毒发病率和病毒载量(VL)抑制率,目前正在将VL检测结果在采集后的八周内反馈给每位艾滋病毒呈阳性参与者指定的医疗机构。我们描述了用于向津巴布韦、马拉维和赞比亚的PHIA参与者反馈VL检测结果的样本及数据管理系统的运行情况。
根据国家检测指南,同意参与的参与者接受了上门咨询和艾滋病毒快速检测;所有确诊为艾滋病毒阳性的参与者都在中央实验室使用罗氏CAP/CTM或雅培m2000平台进行了VL检测。一个专门的数据管理团队每两周生成一次记录,将VL检测结果与参与者的联系信息及首选医疗机构关联起来;项目工作人员通过项目司机、国家快递系统或通过适配的短信服务(SMS)以电子方式将检测结果保密发送出去。提供了手机号码的参与者会收到关于VL检测结果是否可用的短信或电话提醒。
在这三个国家的29634个家庭中,津巴布韦和马拉维共有78090名0至64岁的参与者,赞比亚有78090名0至59岁的参与者接受了采血和艾滋病毒检测。在总共识别出的8391名艾滋病毒阳性参与者中,8313人(99%)进行了VL检测,其中8245人(99%)的检测结果被反馈到了选定的医疗机构。在津巴布韦和赞比亚反馈的5979份VL检测结果中,85%在八周的目标期限内反馈,中位周转时间为48天(四分位距:33至61天)。在马拉维,由于无法获取确切的反馈日期,所有2266份可反馈的结果在11周内都送达了医疗机构。
前三轮PHIA调查在八周目标期限内将绝大多数VL检测结果反馈给了每位艾滋病毒阳性参与者首选的医疗机构。即使没有国家VL监测系统,基于人群调查的VL检测结果反馈系统也是可行的,但这需要建立实验室和数据管理系统以及配备专门的工作人员。这些可能是加强常规临床护理中检测结果反馈系统的重要要求。