Department of Epidemiology, Boston University School of Public Health, Boston, MA, USA.
Department of Global Health, Boston University School of Public Health, Boston, MA, USA.
J Int AIDS Soc. 2020 Jul;23(7):e25542. doi: 10.1002/jia2.25542.
In South Africa, HIV patients with an elevated viral load (VL) should receive repeat VL testing after adherence counselling. We set out to use a national HIV Cohort to describe time to repeat viral load testing across South Africa and identify predictors of time to repeat testing.
We conducted a cohort study of prospectively collected laboratory data. HIV treatment guidelines have changed over time in South Africa, but call for repeat VL testing within six months if 400 to 1000 copies/mL and two to three months if >1000 copies/mL. We included patients with suppressed viral loads (indicating they are on ART) and a first elevated VL (>400 copies/mL) between April 2004 and December 2014. Follow-up began at first elevated VL and continued until repeat testing, loss to follow-up or December 2016. We calculated adjusted hazard ratios (aHR) using Cox proportional hazard models.
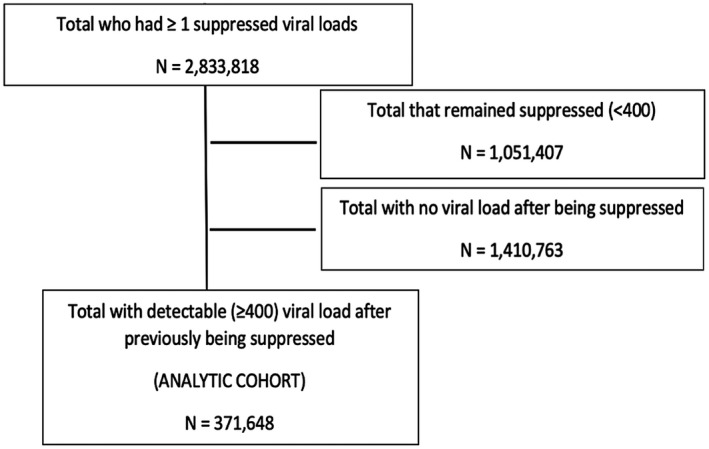
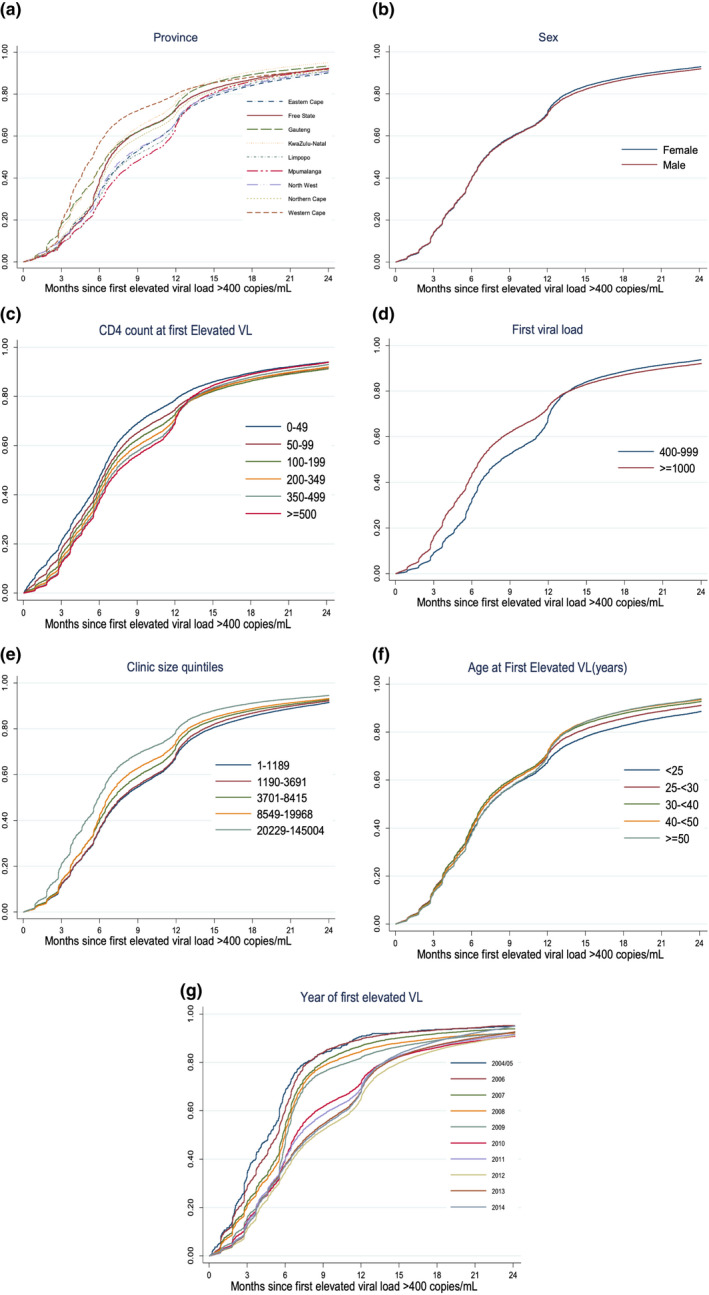
Of 371,648 patients with a VL > 400, 83.9% (311,790) had a repeat VL, in a median (IQR) of 7.0 (4.1 to 12.2) months. Of those with a first viral load 400 to 1000 copies/mL, 56.4% had a repeat VL within guideline recommended six months (defined as up to nine months), whereas among those >1000 copies/mL only 47.7% had a repeat viral load within guideline recommended two to three months (defined as up to six months). We found a small increase in repeat testing associated with higher VL value (aHR 1.11; 95% CI: 1.10 to 1.12 comparing >1000 vs 400 to 1000 copies/mL) and very low CD4 counts at first elevated VL (aHR 1.16; 95% CI: 1.13 to 1.19 comparing CD4 < 50 vs <500 cells/mm ). We also found strong variation in time to repeat VL testing by province.
Median time to repeat viral load testing for those with an elevated viral load was longer than guidelines recommend. Future work should identify whether delays are due to patient or provider factors.
在南非,HIV 患者病毒载量(VL)升高时,应在接受遵嘱服药咨询后重复进行 VL 检测。我们旨在利用全国性 HIV 队列来描述南非各地重复进行病毒载量检测的时间,并确定重复检测时间的预测因素。
我们开展了一项前瞻性采集实验室数据的队列研究。南非的 HIV 治疗指南随时间发生了变化,但如果 VL 为 400 至 1000 拷贝/毫升,则建议在 6 个月内重复进行 VL 检测,如果 VL 大于 1000 拷贝/毫升,则建议在 2 至 3 个月内重复进行 VL 检测。我们纳入了病毒载量得到抑制(表明正在接受 ART 治疗)且首次 VL 升高(>400 拷贝/毫升)的患者,这些患者在 2004 年 4 月至 2014 年 12 月期间入组。随访自首次 VL 升高开始,一直持续至重复检测、失访或 2016 年 12 月。我们使用 Cox 比例风险模型计算了调整后的危险比(aHR)。
在 371648 名 VL 大于 400 拷贝/毫升的患者中,83.9%(311790 名)重复进行了 VL 检测,中位(IQR)时间为 7.0(4.1 至 12.2)个月。对于 VL 为 400 至 1000 拷贝/毫升的患者,56.4%在指南推荐的 6 个月内(定义为最长 9 个月)重复进行了 VL 检测,而对于 VL 大于 1000 拷贝/毫升的患者,只有 47.7%在指南推荐的 2 至 3 个月内(定义为最长 6 个月)重复进行了病毒载量检测。我们发现,VL 值越高(与 VL 为 400 至 1000 拷贝/毫升的患者相比,aHR 为 1.11;95%CI:1.10 至 1.12)和首次 VL 升高时 CD4 计数极低(与 CD4<50 细胞/mm3 的患者相比,aHR 为 1.16;95%CI:1.13 至 1.19)与重复进行 VL 检测的次数增加相关。此外,我们还发现,各省之间重复进行 VL 检测的时间存在明显差异。
对于 VL 升高的患者,重复进行病毒载量检测的中位时间长于指南推荐的时间。未来的研究工作应确定这种延迟是由于患者还是提供者因素导致的。