Kotake Yasuhito, Yasuoka Ryobun, Tanaka Motohide, Noda Takashi, Nitta Takashi, Aizawa Yoshifusa, Ohe Tohru, Nakazawa Gaku, Kurita Takashi
Department of Internal Medicine, Faculty of Medicine, Kindai University, Osaka-Sayama, Japan.
Department of Cardiovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Japan.
Int J Cardiol Heart Vasc. 2020 Dec 31;32:100704. doi: 10.1016/j.ijcha.2020.100704. eCollection 2021 Feb.
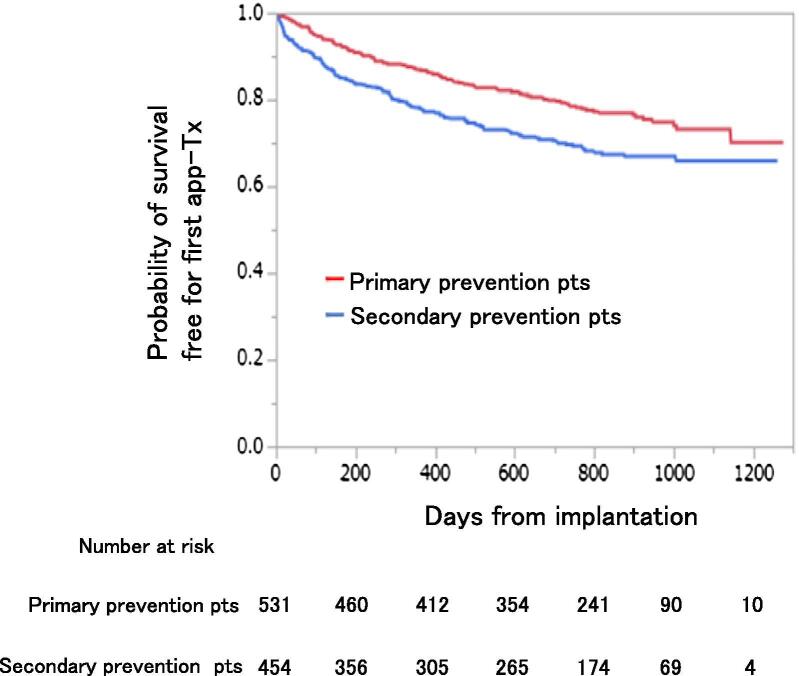
Patients with implantable cardioverter defibrillator (ICD) use for primary prevention (primary prevention patients) of sudden cardiac death have lower incidence of appropriate ICD therapy (app-Tx) compared with those with ICD use for secondary prevention (secondary prevention patients). However, detail analysis of a second app-Tx after a first app-Tx is still lacking.
This study aimed to compare the incidence of a second app-Tx in primary vs secondary prevention patients.
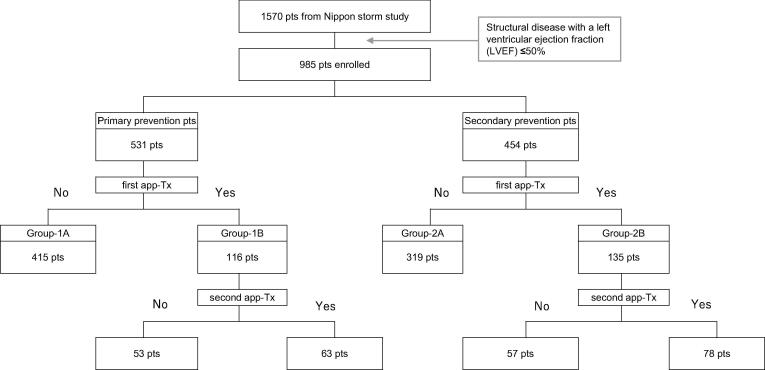
We conducted sub-analysis of the Nippon Storm Study, which was a prospective, observational study involving 985 patients with structural heart disease (left ventricular ejection fraction ≤ 50%). Of these, we selected 251 patients (62 ± 14 years old, 82% men) who experienced at least one appropriate ICD therapy, and compared occurrence of a second app-Tx between primary (n = 116) and secondary (n = 135) prevention patients.
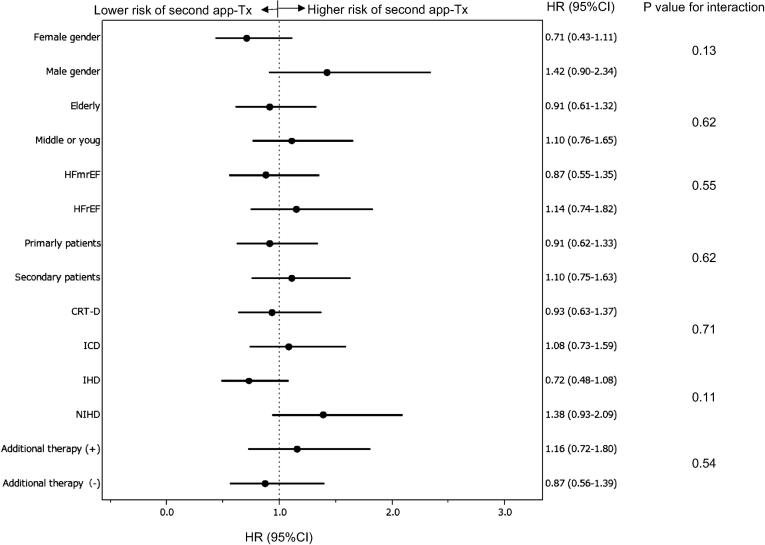
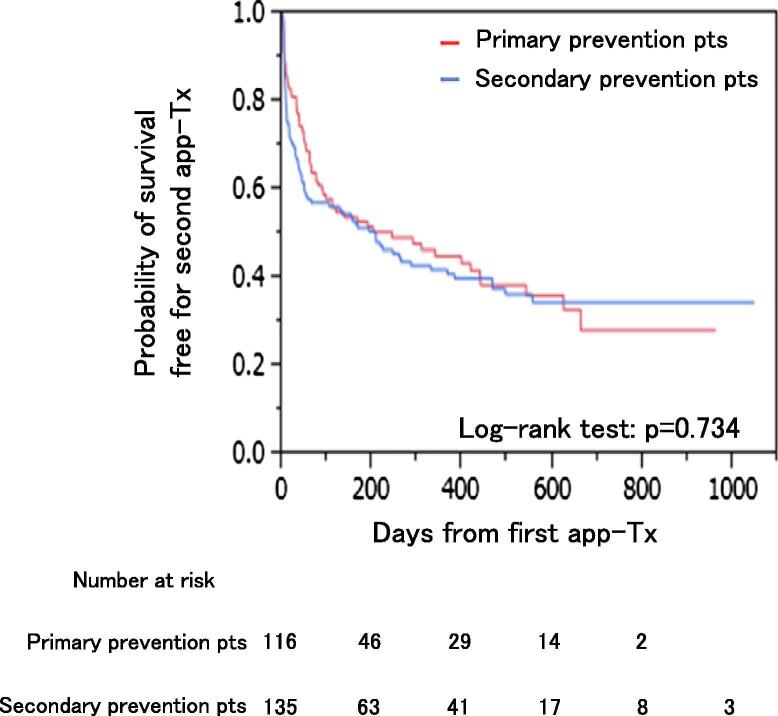
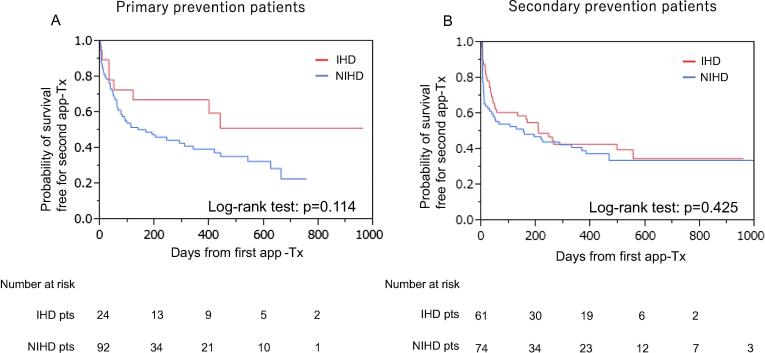
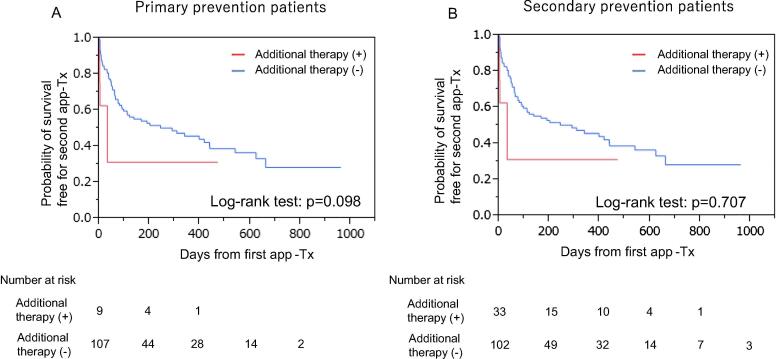
There was no significant difference in the incidence of a second app-Tx between primary and secondary prevention patients (the cumulative incidence for a second app-Tx was 59% at 1 year and 79% at 3 years in primary prevention patients vs the cumulative incidence for the second app-Tx was 59% at 1 year and 75% at 3 years in secondary prevention patients).Additionally, we evaluated the incidence of a second app-Tx according to basal structural disease (ischemic and non-ischemic cardiomyopathy) and found no significant difference between primary and secondary prevention patients.
Once app-Tx occurs, primary prevention patients acquire the high risk of subsequent ventricular arrhythmias because there is a comparable incidence of a second app-Tx in secondary prevention patients.
与用于心脏性猝死二级预防的植入式心律转复除颤器(ICD)患者(二级预防患者)相比,用于心脏性猝死一级预防的ICD患者(一级预防患者)接受适当ICD治疗(恰当治疗)的发生率较低。然而,对于首次恰当治疗后再次发生恰当治疗的详细分析仍很缺乏。
本研究旨在比较一级预防患者与二级预防患者再次发生恰当治疗的发生率。
我们对日本风暴研究进行了亚组分析,这是一项前瞻性观察性研究,纳入了985例结构性心脏病患者(左心室射血分数≤50%)。其中,我们选取了251例至少经历过一次恰当ICD治疗的患者(62±14岁,82%为男性),比较了一级预防患者(n = 116)和二级预防患者(n = 135)再次发生恰当治疗的情况。
一级预防患者与二级预防患者再次发生恰当治疗发生率无显著差异(一级预防患者再次发生恰当治疗的累积发生率在1年时为59%,3年时为79%;二级预防患者再次发生恰当治疗的累积发生率在1年时为59%,3年时为75%)。此外,我们根据基础结构性疾病(缺血性和非缺血性心肌病)评估了再次发生恰当治疗的发生率,发现一级预防患者与二级预防患者之间无显著差异。
一旦发生恰当治疗,一级预防患者随后发生室性心律失常的风险较高,因为二级预防患者再次发生恰当治疗的发生率与之相当。