Gaede Luise, Herchenbach Amanda, Tröbs Monique, Marwan Mohamed, Achenbach Stephan
Friedrich Alexander Universität Erlangen-Nürnberg (FAU), Medizinische Klinik 2, Universitätsklinikum Erlangen, Germany.
Int J Cardiol Heart Vasc. 2021 Jan 6;32:100708. doi: 10.1016/j.ijcha.2020.100708. eCollection 2021 Feb.
Takotsubo Syndrome (TTS) is diagnosed in 1-2% of all patients presenting with acute coronary syndrome. Next to the typical apical manifestation, other locations of left ventricular contraction abnormality are possible, but their relationship to patient characteristics, clinical correlates as well as long-term outcome are poorly understood.
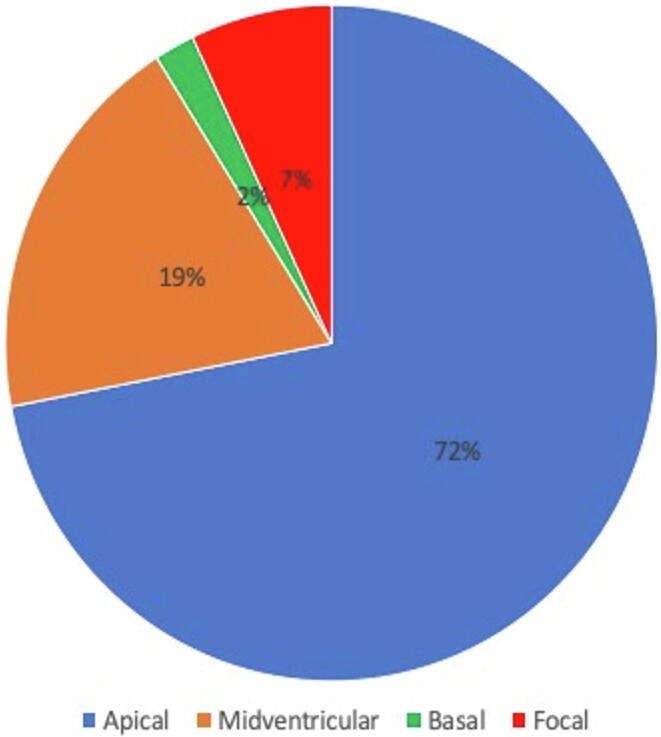
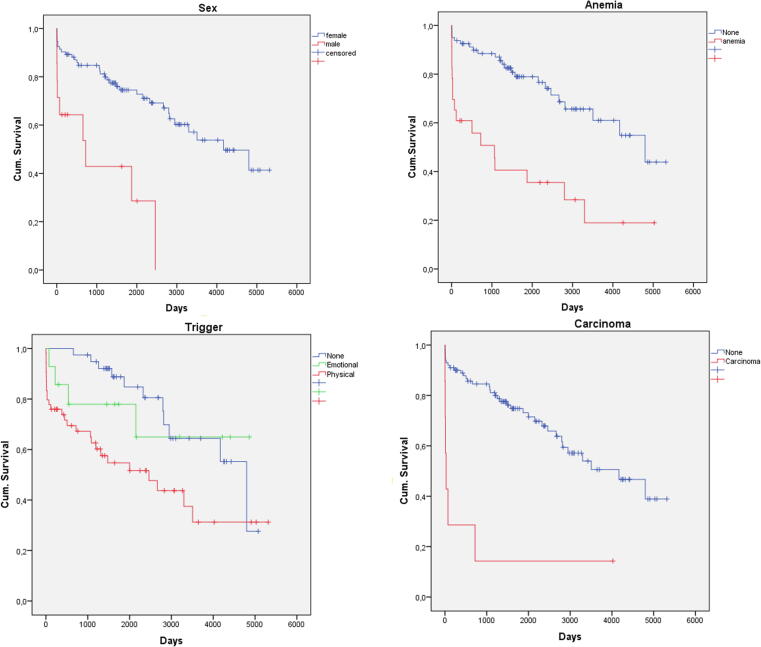
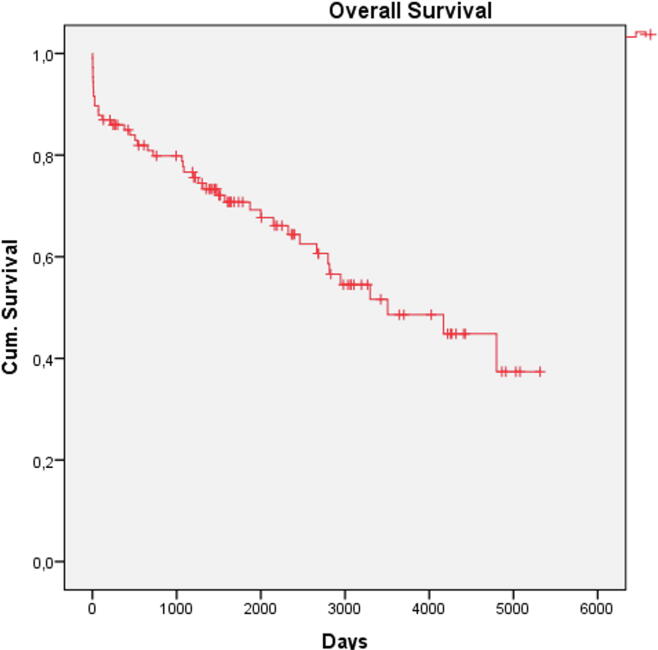
METHODS & RESULTS: We retrospectively analyzed 126 patients presenting TTS. Cases were categorized according to left ventricular contraction abnormality patterns: typical apical pattern (71%, n = 89) vs. atypical patterns (29%, n = 37). Cases with typical TTS showed significantly higher levels of troponin I (3.12 ng/ml vs. 1.32 ng/ml, p = 0.013) and creatin kinase (CK) on admission (461 (±1207)U/l vs. 173 (±177) U/l, p = 0.03) as well as peak CK (973 (±2860)U/l vs. 301 (±328) U/l, p = 0.03) and more often ischemia related ECG changes (p = 0.02). Follow-up data was available for 85% of the patients. Median FU time was 4.4 years (IQR 1.4-7.7 years). All-cause mortality during follow-up was 39%, with no significant difference between patients with typical or atypical TTS (43% vs. 29%, p = 0.17). In multivariate logistic regression analysis, only anemia was predictive for long-term mortality (OR 3.93, 95%CI 1.02-2.08, p = 0.015). The majority of surviving patients (69%) reported good quality of life, even though only 56% reported being symptom-free.
Patients with TTS have poor long-term prognosis with an overall mortality of 39.1% within 4 years and nearly half of all patients report persisting symptoms. Even though the apical contraction pattern is associated with higher elevation of serum markers for myocardial damage, it was not associated with higher long-term mortality.
在所有急性冠脉综合征患者中,1% - 2%被诊断为应激性心肌病(TTS)。除了典型的心尖部表现外,左心室收缩异常的其他部位也有可能出现,但人们对其与患者特征、临床相关因素以及长期预后的关系了解甚少。
我们回顾性分析了126例TTS患者。根据左心室收缩异常模式对病例进行分类:典型心尖部模式(71%,n = 89)与非典型模式(29%,n = 37)。典型TTS患者入院时肌钙蛋白I水平(3.12 ng/ml对1.32 ng/ml,p = 0.013)和肌酸激酶(CK)水平(461(±1207)U/l对173(±177)U/l,p = 0.03)以及CK峰值(973(±2860)U/l对301(±328)U/l,p = 0.03)显著更高,且缺血相关心电图改变更常见(p = 0.02)。85%的患者有随访数据。随访中位时间为4.4年(四分位间距1.4 - 7.7年)。随访期间全因死亡率为39%,典型或非典型TTS患者之间无显著差异(43%对29%,p = 0.17)。在多因素逻辑回归分析中,只有贫血可预测长期死亡率(比值比3.93,95%置信区间1.02 - 2.08,p = 0.015)。大多数存活患者(69%)报告生活质量良好,尽管只有56%报告无症状。
TTS患者长期预后较差,4年内总死亡率为39.1%,近一半患者报告有持续症状。尽管心尖部收缩模式与心肌损伤血清标志物的更高升高有关,但与更高的长期死亡率无关。