Kazda Tomas, Pafundi Deanna H, Kraling Alan, Bradley Thomas, Lowe Val J, Brinkmann Debra H, Laack Nadia N
Department of Radiation Oncology, Faculty of Medicine Masaryk University and Masaryk Memorial Cancer Institute, Brno, Czech Republic.
International Clinical Research Center, St. Anne's University Hospital, Brno, Czech Republic.
Phys Imaging Radiat Oncol. 2018 Jun 22;6:94-100. doi: 10.1016/j.phro.2018.06.004. eCollection 2018 Apr.
The amino-acid positron emission tomography (PET) tracer 3,4-dihydroxy-6-[F] fluoro-l-phenylalanine (F-DOPA) has increased sensitivity for detecting regions of biologically aggressive tumors compared to T1 contrast-enhanced (T1-CE) magnetic resonance imaging (MRI). We performed dosimetric evaluation of treatment plans prepared with and without inclusion of F-DOPA-based biological target volume (BTV) evaluating its role in guiding radiotherapy of grade III/IV gliomas.
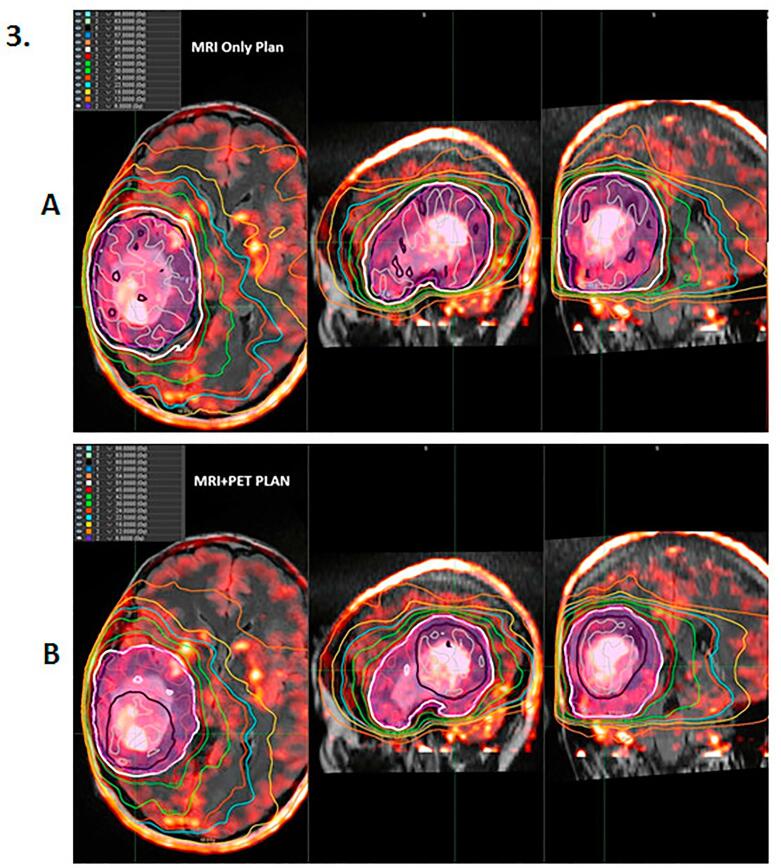
Eight patients (five T1-CE, three non-contrast-enhancing [NCE]) were included in our study. MRI only-guided anatomic plans and MRI+FDOPA-PET-guided biologic plans were prepared for each patient, and dosimetric data for target volumes and organs at risk (OAR) were compared. High-dose BTV was defined as regions with tumor to normal brain (T/N) >2.0, while low-dose BTV was initially based on T/N >1.3, but refined per Nuclear Medicine expert.
For T1-CE tumors, planning target volumes (PTV) were larger than MRI-only anatomic target volumes. Despite increases in size of both gross target volumes and PTV, with volumetric-modulated arc therapy planning, no increase of dose to OAR was observed while maintaining similar target dose coverage. For NCE tumors, MRI+F-DOPA PET biologic imaging identified a sub-region of the large, T2-FLAIR abnormal signal which may allow a smaller volume to receive the high dose (60 Gy) radiation.
For T1-CE tumors, PTVs were larger than MRI-only anatomic target volumes with no increase of dose to OARs. Therefore, MRI+F-DOPA PET-based biologic treatment planning appears feasible in patients with high-grade gliomas.
与T1加权增强(T1-CE)磁共振成像(MRI)相比,氨基酸正电子发射断层扫描(PET)示踪剂3,4-二羟基-6-[F]氟-L-苯丙氨酸(F-DOPA)在检测具有生物学侵袭性的肿瘤区域方面具有更高的灵敏度。我们对包含和不包含基于F-DOPA的生物靶区(BTV)的治疗计划进行了剂量学评估,以评估其在指导III/IV级胶质瘤放疗中的作用。
本研究纳入了8例患者(5例T1-CE,3例无强化[NCE])。为每位患者制定了仅基于MRI的解剖学计划和MRI+FDOPA-PET引导的生物学计划,并比较了靶区体积和危及器官(OAR)的剂量学数据。高剂量BTV定义为肿瘤与正常脑(T/N)>2.0的区域,而低剂量BTV最初基于T/N>1.3,但由核医学专家进行了细化。
对于T1-CE肿瘤,计划靶区体积(PTV)大于仅基于MRI的解剖学靶区体积。尽管大体靶区体积和PTV均增大,但在容积调强弧形放疗计划中,在维持相似靶区剂量覆盖的同时,未观察到OAR剂量增加。对于NCE肿瘤,MRI+F-DOPA PET生物学成像识别出大的T2-FLAIR异常信号中的一个子区域,这可能使较小体积的区域接受高剂量(60 Gy)辐射。
对于T1-CE肿瘤,PTV大于仅基于MRI的解剖学靶区体积,且OAR剂量未增加。因此,基于MRI+F-DOPA PET的生物学治疗计划在高级别胶质瘤患者中似乎是可行的。