Christiansen Rasmus Lübeck, Hansen Christian Rønn, Dahlrot Rikke Hedegaard, Bertelsen Anders Smedegaard, Hansen Olfred, Brink Carsten, Bernchou Uffe
Laboratory of Radiation Physics, Odense University Hospital, DK-5000 Odense, Denmark.
Institute of Clinical Research, University of Southern Denmark, DK-5000 Odense, Denmark.
Phys Imaging Radiat Oncol. 2018 Jul 21;7:1-8. doi: 10.1016/j.phro.2018.06.006. eCollection 2018 Jul.
Daily radiotherapy plan adaptation facilitated by a high field magnetic resonance linac (MRL) may potentially reduce the treated volume due to a reduction of the setup uncertainty. However, the technology also imposes limitations to the treatment technique compared to a standard linac. This study investigated the clinical quality of MRL treatment plans against current standard plans using identical planning target volume margins for high-risk prostate cancer patients.
Twenty consecutive patients planned with our current clinical standard TPS and treated with single arc VMAT on standard linacs with 78 Gy in the prostate and 56 Gy for pelvic lymph nodes over 39 fractions were included. In addition, IMRT treatment plans for delivery by a 1.5 T MRL, using standard margins and dose objectives, were made in a dedicated TPS. Mean population dose volume histograms (DVH) and dose metrics were analyzed and clinical plan quality was evaluated by an oncologist.
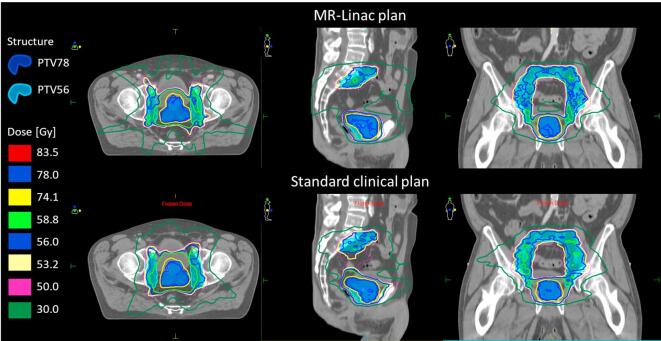
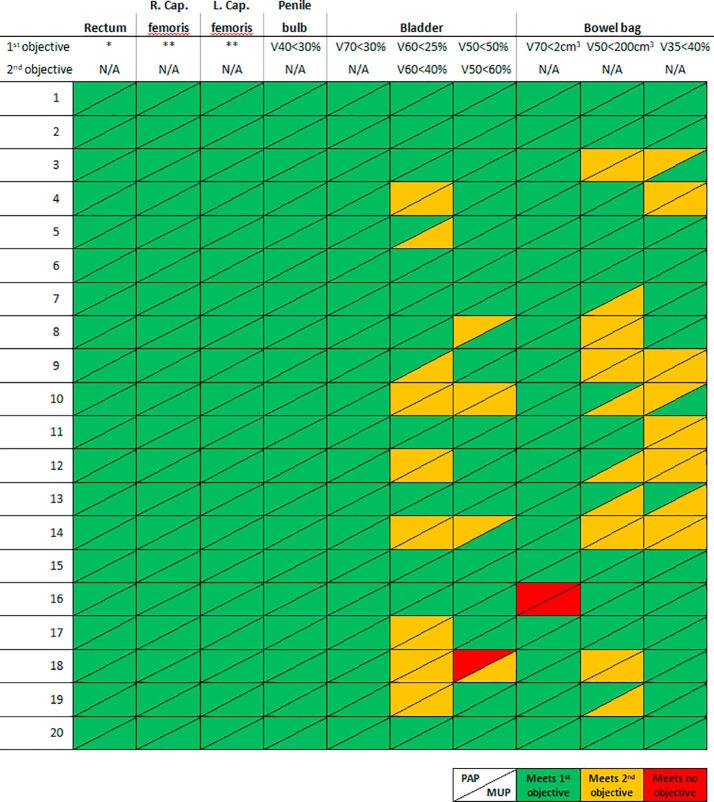
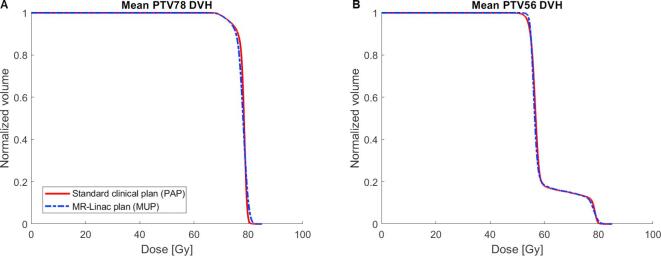
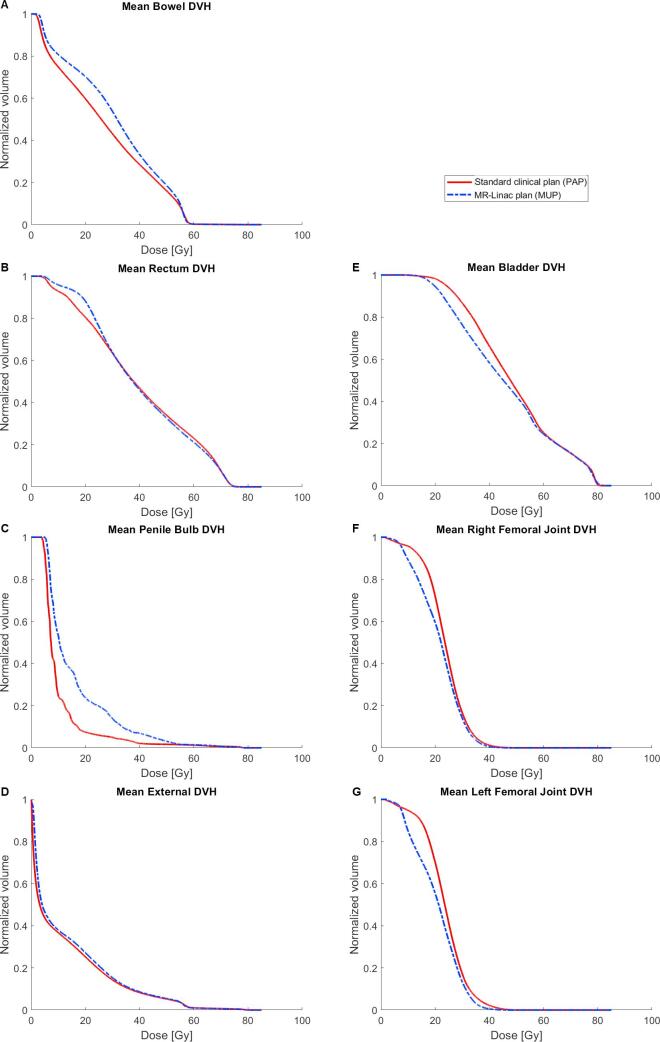
All MRL plans were considered clinically acceptable, and DVH analysis showed an overall high similarity to dose distributions of the clinically delivered plans. Mean target coverage was similar (78.0 Gy vs 77.8 Gy). Small but statistically significant differences were seen in doses to organs at risk; on average MRL plans reduced dose to the bladder (46.2 vs 48.3 Gy) compared to standard plans, while dose was higher to the bowel (29.2 vs 26.6 Gy) and penile bulb (16.5 vs 10.8 Gy).
MRL treatment plans were clinically acceptable and similar in quality to the current standard.
高场磁共振直线加速器(MRL)辅助的每日放疗计划适应性调整,可能会因设置不确定性的降低而潜在地减少治疗体积。然而,与标准直线加速器相比,该技术也对治疗技术施加了限制。本研究针对高危前列腺癌患者,使用相同的计划靶体积边界,对比了MRL治疗计划与当前标准计划的临床质量。
纳入连续20例采用我们当前临床标准治疗计划系统进行计划,并在标准直线加速器上接受单次弧VMAT治疗的患者,前列腺剂量为78Gy,盆腔淋巴结剂量为56Gy,分39次照射。此外,在专用治疗计划系统中制定了使用标准边界和剂量目标的、由1.5T MRL进行照射的调强放射治疗(IMRT)计划。分析了平均总体剂量体积直方图(DVH)和剂量指标,并由一名肿瘤学家评估临床计划质量。
所有MRL计划均被认为在临床上可接受,DVH分析显示其与临床实施计划的剂量分布总体高度相似。平均靶区覆盖相似(78.0Gy对77.8Gy)。在危及器官的剂量方面观察到虽小但具有统计学意义的差异;与标准计划相比,MRL计划平均降低了膀胱剂量(46.2对48.3Gy),而肠道剂量(29.2对26.6Gy)和阴茎球部剂量(16.5对10.8Gy)更高。
MRL治疗计划在临床上可接受,质量与当前标准相似。