Arscott W Tristram, Thompson Reid F, Yin Lingshu, Burgdorf Brendan, Kirk Maura, Ben-Josef Edgar
Department of Radiation Oncology, Hospital of the University of Pennsylvania, United States.
Department of Radiation Medicine, Oregon Health & Science University, Portland VA Healthcare System, United States.
Phys Imaging Radiat Oncol. 2018 Nov 22;8:17-22. doi: 10.1016/j.phro.2018.11.004. eCollection 2018 Oct.
Photon Stereotactic Body Radiotherapy (SBRT) for primary and metastatic tumors of the liver is challenging for larger lesions. An comparison of paired SBRT and Stereotactic Body Proton Therapy (SBPT) plans was performed to understand the potential advantages of SBPT as a function of tumor size and location.
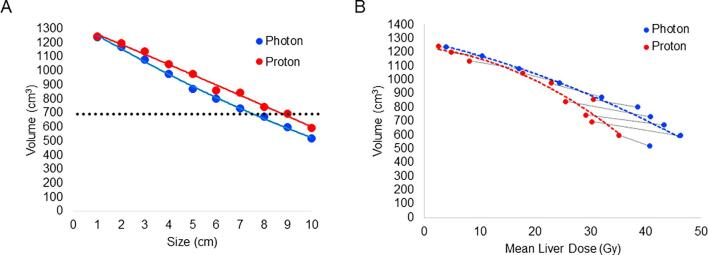
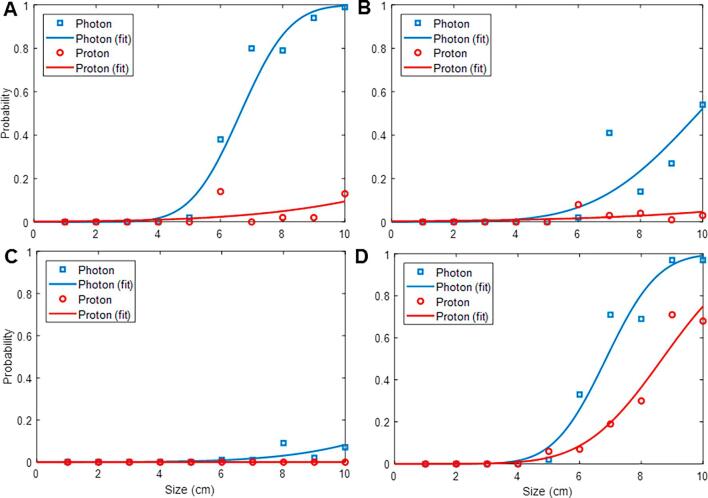
Theoretical tumor volumes with maximum diameter of 1-10 cm were contoured in the dome, right inferior, left medial, and central locations. SBRT and SBPT plans were generated to deliver 50 Gy in 5 fractions, max dose <135%. When organs-at-risk (OAR) constraints were exceeded, hypothetical plans (not clinically acceptable) were generated for comparison. Liver normal tissue complication probability (NTCP) models were applied to evaluate differences between treatment modalities.
SBRT and SBPT were able to meet target goals and OAR constraints for lesions up to 7 cm and 9 cm diameter, respectively. SBPT plans resulted in a higher integral gross target dose for all lesions up to 7 cm (mean dose 57.8 ± 2.3 Gy to 64.1 ± 2.2 Gy, < 0.01). Simultaneously, SBPT spared dose to the uninvolved liver in all locations (from 11.5 ± 5.3 Gy to 8.6 ± 4.4 Gy, < 0.01), resulting in lower NTCP particularly for larger targets in the dome and central locations. SBPT also spared duodenal dose across all sizes and positions (from 7.3 ± 1.1 Gy to 1.1 ± 0.3 Gy, < 0.05).
The main advantages of SBPT over SBRT is meeting plan goals and constrains for larger targets, particularly dome and central locations, and sparing dose to uninvolved liver. For such patients, SBPT may allow improvements in tumor control and treatment safety.
对于肝脏原发性和转移性肿瘤,光子立体定向体部放射治疗(SBRT)在治疗较大病灶时具有挑战性。本研究对配对的SBRT和立体定向体部质子治疗(SBPT)计划进行比较,以了解SBPT在肿瘤大小和位置方面的潜在优势。
在肝顶、右下、左中及中央位置勾勒出最大直径为1 - 10厘米的理论肿瘤体积。生成SBRT和SBPT计划,分5次给予50 Gy,最大剂量<135%。当超出危及器官(OAR)限制时,生成假设计划(临床不可接受)用于比较。应用肝脏正常组织并发症概率(NTCP)模型评估不同治疗方式之间的差异。
SBRT和SBPT分别能够满足直径达7厘米和9厘米病灶的靶区目标及OAR限制。对于所有直径达7厘米的病灶,SBPT计划的总靶区积分剂量更高(平均剂量从57.8±2.3 Gy至64.1±2.2 Gy,P<0.01)。同时,SBPT在所有位置均减少了对未受累肝脏的剂量(从11.5±5.3 Gy降至8.6±4.4 Gy,P<0.01),尤其对于肝顶和中央位置的较大靶区,NTCP更低。SBPT在所有大小和位置也减少了十二指肠剂量(从7.3±1.1 Gy降至1.1±0.3 Gy,P<0.05)。
SBPT相对于SBRT的主要优势在于能够满足更大靶区(尤其是肝顶和中央位置)的计划目标和限制,并减少对未受累肝脏的剂量。对于此类患者,SBPT可能会改善肿瘤控制和治疗安全性。