Lambrecht Marie, Sonke Jan-Jakob, Nestle Ursula, Peulen Heike, Weber Damien C, Verheij Marcel, Hurkmans Coen W
Department of Radiation Oncology, Catharina Hospital, Eindhoven, The Netherlands.
Department of Radiation Oncology, The Netherland Cancer Institute, Amsterdam, The Netherlands.
Phys Imaging Radiat Oncol. 2018 Dec 7;8:57-62. doi: 10.1016/j.phro.2018.10.003. eCollection 2018 Oct.
Extensive radiation therapy quality assurance (RTQA) programs are needed when advanced radiotherapy treatments are used. As part of the RTQA four dimensional computed tomography (4DCT) imaging performance needs to be assessed. Here we present the RTQA data related to 4DCT procedures used within the context of stereotactic body radiotherapy (SBRT) of centrally located lung tumours. It provides an overview of the 4DCT acquisition methods and achievable accuracy of imaging lung tumour volumes.
3DCT and 4DCT images were acquired from a CIRS phantom with spheres of 7.5 and 12.5 mm radius using the institutional scan protocols. Regular asymmetric tumour motion was simulated with varying amplitudes and periods. Target volumes were reconstructed using auto-contouring with scanner specific thresholds. Volume and amplitudes deviations were assessed.
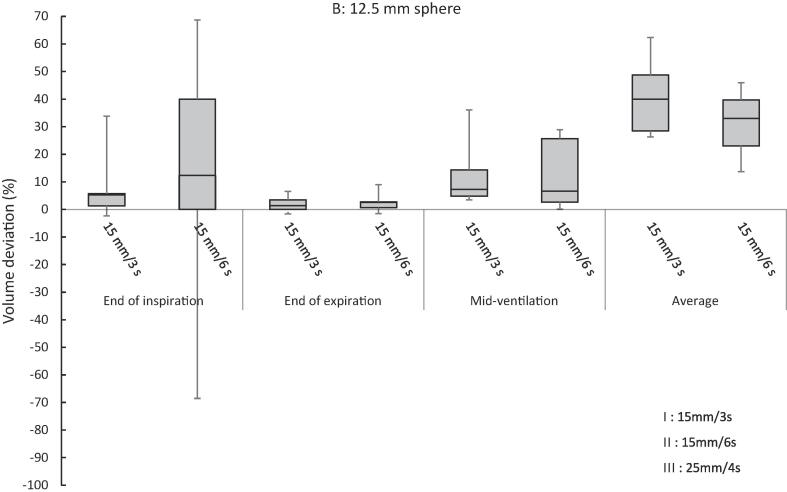
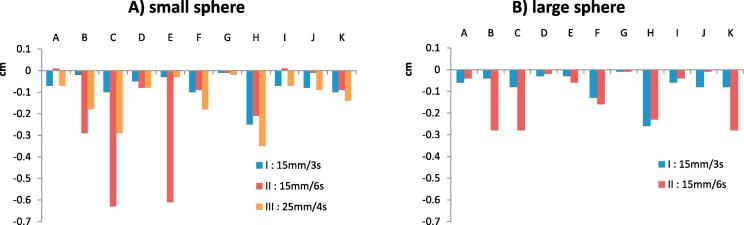
Although acquisition parameters were rather homogeneous over the eleven institutions analysed, volume deviations were observed. Average volume deviations for the 12.5 mm sphere were 15% (-4% to 69%) at end of inspiration, 2% (-2% to 9.0%) at end of expiration and 12% (0% to 36%) at mid-ventilation. For the 7.5 mm sphere deviations were 13% (-99% to 65%), 16% (-34% to 66%) and 1% (-13% to 20%), respectively. The amplitude deviation was generally within 2 mm although underestimations up to 6 mm were observed.
The expiration phase was the most accurate phase to define the tumour volume and should be preferred for GTV delineation of tumours exhibiting large motion causing motion artefacts when using mid-ventilation or tracking techniques. The large variation found among the institutions indicated that further improvements in 4DCT imaging were possible. Recommendations for 4DCT QA have been formulated.
当采用先进的放射治疗方法时,需要广泛的放射治疗质量保证(RTQA)计划。作为RTQA的一部分,需要评估四维计算机断层扫描(4DCT)成像性能。在此,我们展示了与位于中央的肺肿瘤立体定向体部放射治疗(SBRT)中使用的4DCT程序相关的RTQA数据。它概述了4DCT采集方法以及成像肺肿瘤体积可达到的准确性。
使用机构扫描协议,从具有半径为7.5和12.5毫米球体的CIRS体模获取3DCT和4DCT图像。模拟具有不同幅度和周期的规则不对称肿瘤运动。使用扫描仪特定阈值的自动轮廓重建靶体积。评估体积和幅度偏差。
尽管在所分析的11个机构中采集参数相当均匀,但仍观察到体积偏差。12.5毫米球体在吸气末的平均体积偏差为15%(-4%至69%),呼气末为2%(-2%至9.0%),通气中期为12%(0%至36%)。对于7.5毫米球体,偏差分别为13%(-99%至65%)、16%(-34%至66%)和1%(-13%至20%)。幅度偏差一般在2毫米以内,尽管观察到高达6毫米的低估情况。
呼气期是定义肿瘤体积最准确的阶段,对于使用通气中期或跟踪技术时表现出大运动导致运动伪影的肿瘤,在勾画大体肿瘤体积(GTV)时应优先选择。各机构之间发现的较大差异表明4DCT成像有可能进一步改进。已制定了4DCT质量保证的建议。