Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, Baylor College of Medicine, Houston, Texas, USA.
Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, Baylor College of Medicine, Houston, Texas, USA
BMJ Case Rep. 2021 Jan 18;14(1):e238863. doi: 10.1136/bcr-2020-238863.
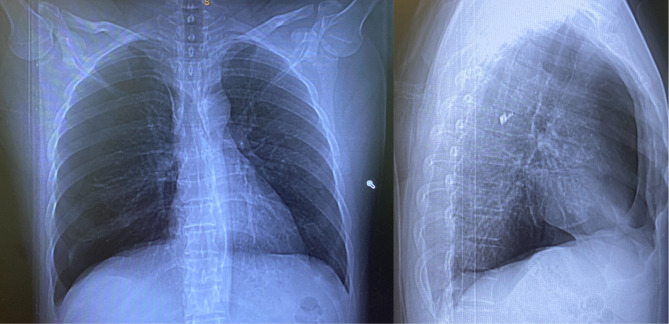
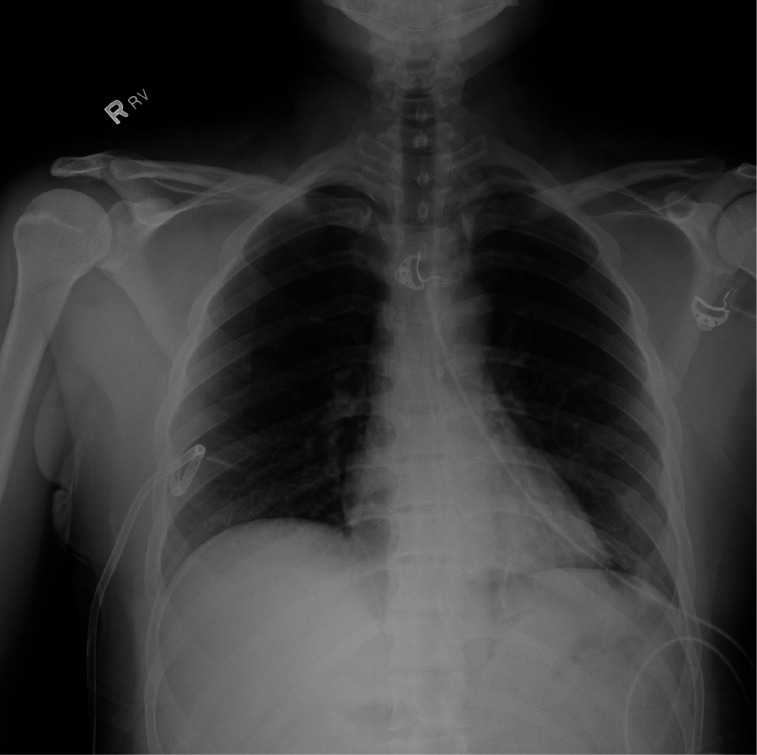
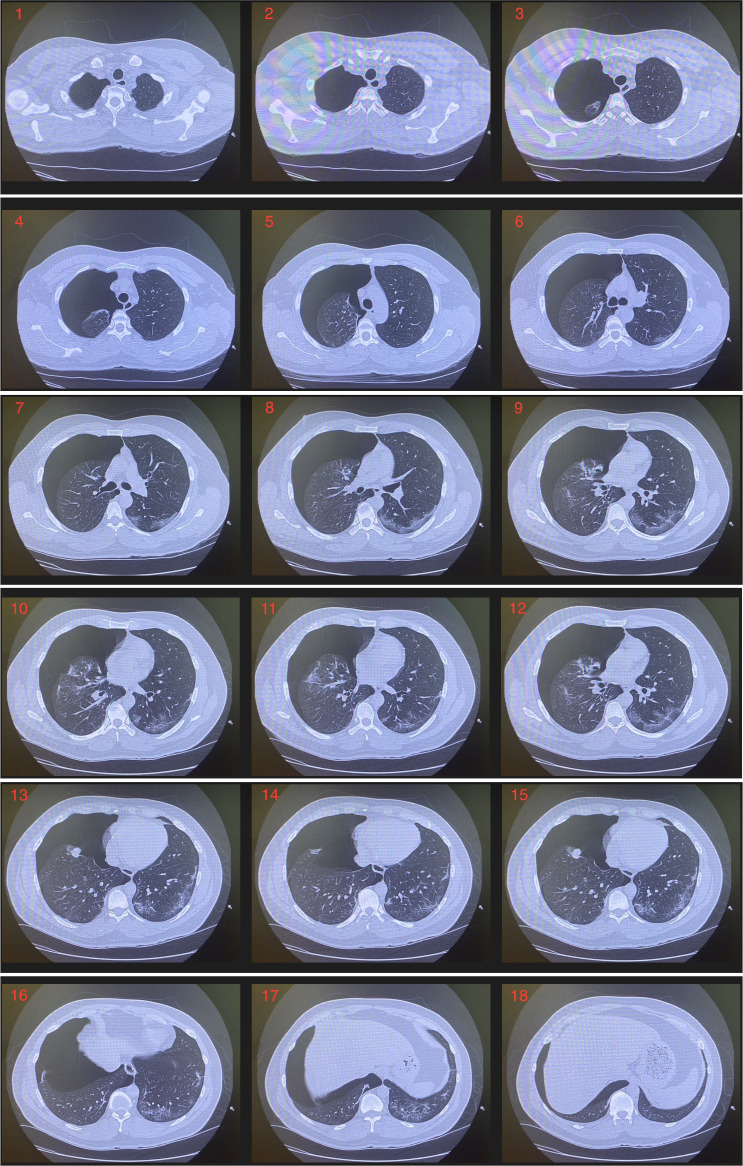
A previously healthy 37-year-old man presented with fevers and myalgias for a week with a minimal dry cough. Initial SARS-CoV-2 nasopharyngeal testing was negative, but in light of high community prevalence, he was diagnosed with COVID-19, treated with supportive care and self-quarantined at home. Three days after resolution of all symptoms, he developed sudden onset chest pain. Chest imaging revealed a large right-sided pneumothorax and patchy subpleural ground glass opacities. IgM and IgG antibodies for SARS-CoV-2 were positive. His pneumothorax resolved after placement of a small-bore chest tube, which was removed after 2 days.This case demonstrates that patients with COVID-19 can develop a significant pulmonary complication, a large pneumothorax, despite only minimal lower respiratory tract symptoms and after resolution of the original illness. Medical professionals should consider development of a pneumothorax in patients who have recovered from COVID-19 and present with new respiratory symptoms.
一位 37 岁既往健康的男性,发热伴肌痛一周,伴有轻微干咳。最初的 SARS-CoV-2 鼻咽拭子检测为阴性,但鉴于社区高发病率,他被诊断为 COVID-19,给予支持性治疗并在家中进行自我隔离。所有症状消退 3 天后,他突发胸痛。胸部影像学显示右侧大量气胸和斑片状胸膜下磨玻璃影。SARS-CoV-2 的 IgM 和 IgG 抗体阳性。他的气胸在放置小口径胸腔引流管后得到缓解,2 天后拔除。该病例表明,即使仅有轻微的下呼吸道症状且原有疾病已痊愈,COVID-19 患者仍可能发生严重的肺部并发症,即大量气胸。因此,对于已从 COVID-19 中康复但出现新的呼吸道症状的患者,临床医生应考虑气胸的发生。