Department of Cell and Molecular Biology, University of Mississippi Medical Center, Jackson, Mississippi.
Department of Medicine, University of Mississippi Medical Center, Jackson, Mississippi.
Am J Physiol Renal Physiol. 2021 Feb 1;320(2):F243-F248. doi: 10.1152/ajprenal.00601.2020. Epub 2021 Jan 19.
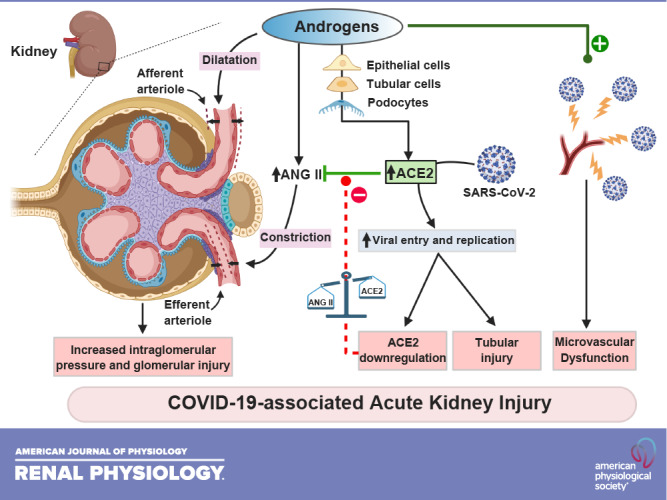
Coronavirus disease 2019 (COVID-19) has reached pandemic proportions, affecting millions of people worldwide. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) is the causative agent of COVID-19. Epidemiological reports have shown that the severity of SARS-CoV-2 infection is associated with preexisting comorbidities such as hypertension, diabetes mellitus, cardiovascular diseases, and chronic kidney diseases, all of which are also risk factors for acute kidney injury (AKI). The kidney has emerged as a key organ affected by SARS-CoV-2. AKI is associated with increased morbidity and mortality in patients with COVID-19. Male sex is an independent predictor for AKI, and an increased death rate has been reported in male patients with COVID-19 worldwide. The mechanism(s) that mediate the sex discrepancy in mortality due to COVID-19 remain(s) unknown. Angiotensin-converting enzyme (ACE)2 is the receptor for SARS-CoV-2. Alterations in the ACE-to-ACE2 ratio have been implicated in renal diseases. This perspective aims to discuss data that suggest that androgens, via alterations in the intrarenal renin-angiotensin system, impair renal hemodynamics, predisposing patients to AKI during COVID-19 infection, which could explain the higher mortality observed in men with COVID-19. Clinicians should ensure early and effective cardiometabolic control for all patients to ameliorate the compensatory elevation of ACE2 and alterations in the ACE-to-ACE2 ratio. A better understanding of the role of androgens in SARS-CoV-2-associated AKI and mortality is imperative. The kidney could constitute a key organ that may explain the sex disparities of the higher mortality and worst outcomes associated with COVID-19 in men.
新型冠状病毒病(COVID-19)已达到大流行的程度,影响了全球数百万人。严重急性呼吸综合征冠状病毒-2(SARS-CoV-2)是 COVID-19 的病原体。流行病学报告表明,SARS-CoV-2 感染的严重程度与高血压、糖尿病、心血管疾病和慢性肾脏病等先前存在的合并症有关,所有这些合并症也是急性肾损伤(AKI)的危险因素。肾脏已成为受 SARS-CoV-2 影响的关键器官。AKI 与 COVID-19 患者的发病率和死亡率增加有关。男性是 AKI 的独立预测因素,据报道,全球 COVID-19 男性患者的死亡率更高。介导 COVID-19 导致死亡率性别差异的机制尚不清楚。血管紧张素转换酶(ACE)2 是 SARS-CoV-2 的受体。肾素-血管紧张素系统(RAS)中 ACE 与 ACE2 比值的改变与肾脏疾病有关。本观点旨在讨论表明雄激素通过改变肾内 RAS,损害肾脏血流动力学,使患者在 COVID-19 感染期间易发生 AKI 的相关数据,这可以解释 COVID-19 男性患者死亡率较高的原因。临床医生应确保所有患者进行早期和有效的代谢控制,以改善 ACE2 的代偿性升高和 ACE 与 ACE2 比值的改变。更好地了解雄激素在 SARS-CoV-2 相关 AKI 和死亡率中的作用至关重要。肾脏可能是一个关键器官,可以解释 COVID-19 男性患者死亡率较高和预后较差的性别差异。