Migdady Ibrahim, Amin Moein, Shoskes Aaron, Hassett Catherine, Cho Sung-Min, George Pravin, Rae-Grant Alexander
Division of Neurocritical Care, Department of Neurology, Massachusetts General Hospital, Harvard Medical School, 55 Fruit Street, Lunder 650, Boston, MA, 02114, USA.
Department of Neurology, Neurological Institute, Cleveland Clinic, Cleveland, OH, USA.
J Intensive Care. 2021 Jan 20;9(1):13. doi: 10.1186/s40560-020-00522-8.
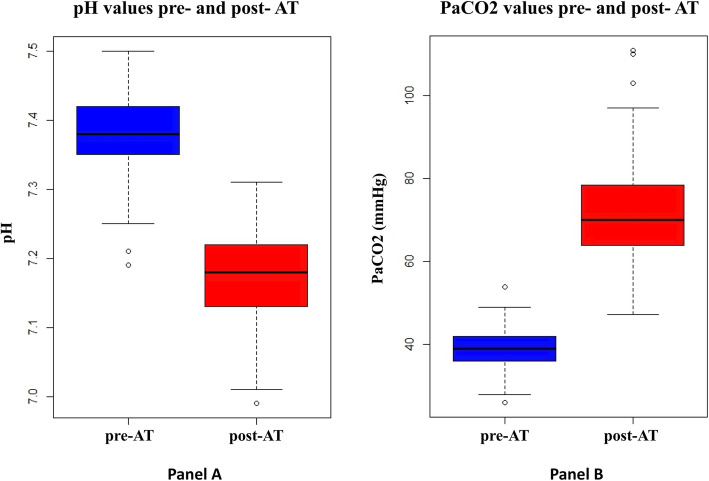
Persistent apnea despite an adequate rise in arterial pressure of CO is an essential component of the criteria for brain death (BD) determination. Current guidelines vary regarding the utility of arterial pH changes during the apnea test (AT). We aimed to study the effect of incorporating an arterial pH target < 7.30 during the AT (in addition to the existing PaCO threshold) on brain death declarations.
We performed retrospective analysis of consecutive adult patients who were diagnosed with BD and underwent AT at the Cleveland Clinic over the last 10 years. Data regarding baseline and post-AT blood gas analyses were collected and analyzed.
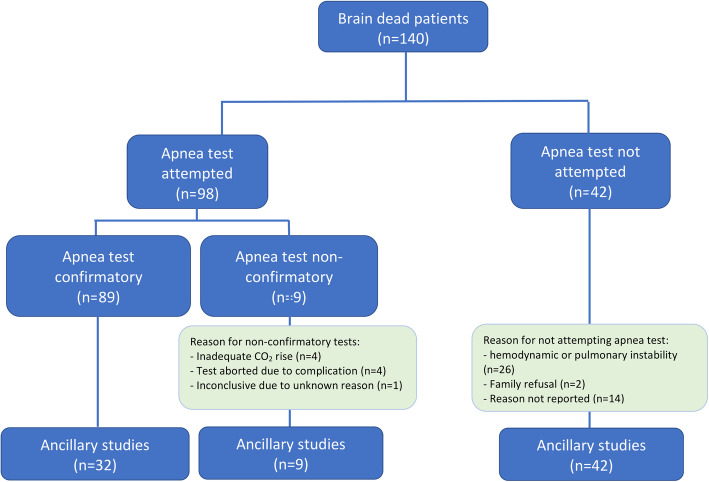
Ninety-eight patients underwent AT in the study period, which was positive in 89 (91%) and inconclusive in 9 (9%) patients. The mean age was 50 years old (standard deviation [SD] 16) and 54 (55%) were female. The most common etiology BD was hypoxic ischemic brain injury (HIBI) due to cardiac arrest (42%). Compared to those with positive AT, patients with inconclusive AT had a higher post-AT pH (7.24 vs 7.17, p = 0.01), lower PaO (47 vs 145, p < 0.01), and a lower PaCO (55 vs 73, p = 0.01). Among patients with a positive AT using PaCO threshold alone, the frequency of patients with post-AT pH < 7.30 was 95% (83/87).
Implementing a BD criteria requiring both arterial pH and PaCO thresholds reduced the total number of positive ATs; these inconclusive cases would have required longer duration of AT to reach both targets, repeated ATs, or ancillary studies to confirm BD. The impact of this on the overall number BD declarations requires further research.
尽管动脉血二氧化碳分压(PaCO₂)有足够升高但仍持续存在呼吸暂停是脑死亡(BD)判定标准的重要组成部分。目前关于呼吸暂停试验(AT)期间动脉血pH值变化的作用,各指南存在差异。我们旨在研究在AT期间纳入动脉血pH目标值<7.30(除现有的PaCO₂阈值外)对脑死亡判定的影响。
我们对过去10年在克利夫兰诊所被诊断为BD并接受AT的成年连续患者进行了回顾性分析。收集并分析了关于基线和AT后血气分析的数据。
在研究期间,98例患者接受了AT,其中89例(91%)结果为阳性,9例(9%)结果不确定。平均年龄为50岁(标准差[SD]16),54例(55%)为女性。BD最常见的病因是心脏骤停导致的缺氧缺血性脑损伤(HIBI)(42%)。与AT结果为阳性的患者相比,AT结果不确定的患者AT后pH值更高(7.24对7.17,p = 0.01),PaO₂更低(47对145,p < 0.01),PaCO₂更低(55对73,p = 0.01)。在仅使用PaCO₂阈值判定为阳性的AT患者中,AT后pH<7.30的患者频率为95%(83/87)。
实施同时要求动脉血pH值和PaCO₂阈值的BD标准减少了AT阳性的总数;这些不确定的病例需要更长时间的AT才能达到两个目标,重复进行AT或进行辅助研究以确认BD。这对总体BD判定数量的影响需要进一步研究。