Tom Baker Cancer Centre, University of Calgary, Calgary, Alberta, Canada.
Department of Medical Oncology, University Hospital 12 de Octubre, Madrid, Spain.
JAMA Netw Open. 2021 Jan 4;4(1):e2021869. doi: 10.1001/jamanetworkopen.2020.21869.
There exists considerable biological and clinical variability between histologic variants of metastatic renal cell carcinoma (mRCC). Data reporting on patterns of metastasis in histologic variants of mRCC are sparse.
To characterize sites of metastasis and their association with survival across the 3 most common histologic variants of mRCC: clear cell (ccRCC), papillary (pRCC), and chromophobe (chrRCC).
DESIGN, SETTING, AND PARTICIPANTS: In this multicenter, international cohort study, the International mRCC Database Consortium (IMDC) database was used to identify consecutive patients starting systemic therapy for mRCC between 2002 and 2019. Patients with mixed histologic subtype were excluded. Statistical analysis was performed from February to June 2020.
Data regarding histologic subtype and sites of metastatic involvement at the time of first systemic therapy initiation were collected.
The primary outcomes were prevalence of metastatic site involvement and overall survival (OS) from time of systemic therapy initiation. Patients with multiple sites of metastatic involvement were included in analyses of all groups to which they had metastases.
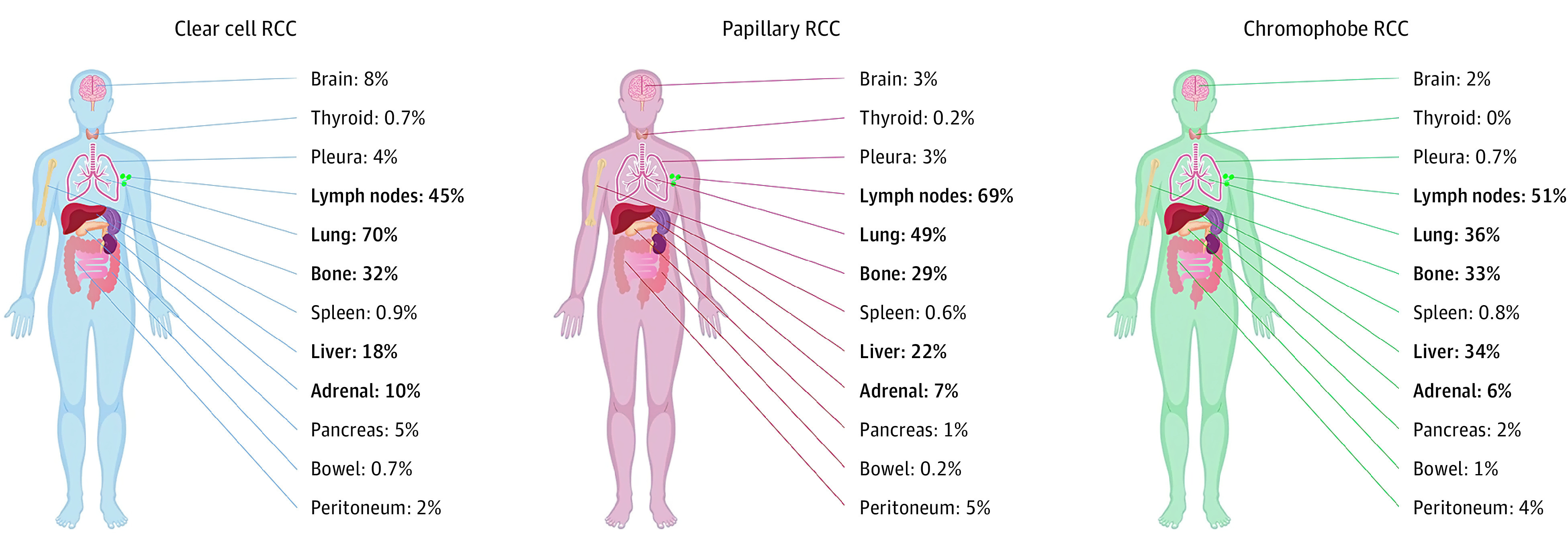
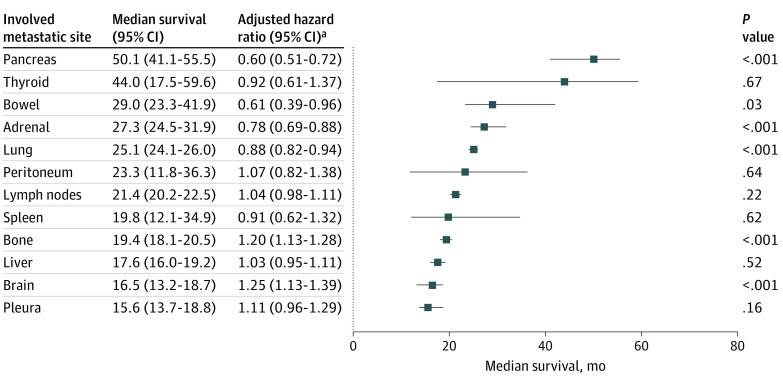
A total of 10 105 patients were eligible for analysis. Median (interquartile range) age at diagnosis was 60 (53-67) years, 7310 (72.4%) were men and 8526 (84.5%) underwent nephrectomy. Of these, 9252 (92%) had ccRCC, 667 (7%) had pRCC, and 186 (2%) had chrRCC. The median number of sites of metastasis was 2 (range, 0-7). In ccRCC, the most common sites of metastasis were lung (70%; 6189 of 8804 patients [448 missing]), lymph nodes (45%; 3874 of 8655 patients [597 missing]), bone (32%; 2847 of 8817 patients [435 missing]), liver (18%; 1560 of 8804 [448 missing]), and adrenal gland (10%; 678 of 6673 patients [2579 missing]). Sites of metastasis varied between subtypes. Lung, adrenal, brain, and pancreatic metastases were more frequent in ccRCC, lymph node involvement was more common in pRCC, and liver metastases were more frequent in chrRCC. Median OS for ccRCC varied by site of metastatic involvement, ranging between 16 months (95% CI, 13.7-18.8 months) for the pleura and 50 months (95% CI, 41.1-55.5 months) for the pancreas. Compared with ccRCC, patients with pRCC tended to have lower OS, regardless of metastatic site.
Sites of metastatic involvement differ according to histologic subtype in mRCC and are associated with OS. These data highlight the clinical and biological variability between histologic subtypes of mRCC. Patterns of metastatic spread may reflect differences in underlying disease biology. Further work to investigate differences in immune, molecular, and genetic profiles between metastatic sites and histologic subtypes is encouraged.
转移性肾细胞癌(mRCC)的组织学变异体之间存在相当大的生物学和临床变异性。关于 mRCC 组织学变异体中转移模式的数据报告很少。
描述最常见的 3 种 mRCC 组织学变异体(透明细胞癌 [ccRCC]、乳头状癌 [pRCC] 和嫌色细胞癌 [chrRCC])中转移部位及其与生存的关系。
设计、地点和参与者:在这项多中心、国际队列研究中,国际 mRCC 数据库联盟(IMDC)数据库用于确定 2002 年至 2019 年期间开始系统治疗的 mRCC 连续患者。排除混合组织学亚型的患者。统计分析于 2020 年 2 月至 6 月进行。
收集首次全身治疗时组织学亚型和转移部位的数据。
主要结局是转移性部位受累的患病率和全身治疗开始时的总生存(OS)。有多个转移部位的患者在所有有转移的组中均进行了分析。
共有 10105 名患者符合分析条件。诊断时的中位(四分位距)年龄为 60 岁(53-67 岁),7310 名(72.4%)为男性,8526 名(84.5%)接受了肾切除术。其中,9252 名(92%)为 ccRCC,667 名(7%)为 pRCC,186 名(2%)为 chrRCC。转移部位的中位数为 2 个(范围,0-7)。在 ccRCC 中,最常见的转移部位是肺(70%;8804 名患者中有 6189 名 [448 名缺失])、淋巴结(45%;8655 名患者中有 3874 名 [597 名缺失])、骨(32%;8817 名患者中有 2847 名 [435 名缺失])、肝(18%;8804 名患者中有 1560 名 [448 名缺失])和肾上腺(10%;6673 名患者中有 678 名 [2579 名缺失])。亚型之间转移部位不同。肺、肾上腺、脑和胰腺转移在 ccRCC 中更为常见,淋巴结受累在 pRCC 中更为常见,而肝转移在 chrRCC 中更为常见。ccRCC 的中位 OS 因转移部位而异,范围从胸膜的 16 个月(95%CI,13.7-18.8 个月)到胰腺的 50 个月(95%CI,41.1-55.5 个月)。与 ccRCC 相比,无论转移部位如何,pRCC 患者的 OS 往往较低。
mRCC 不同组织学亚型的转移部位不同,与 OS 相关。这些数据突出了 mRCC 组织学亚型之间的临床和生物学变异性。转移扩散模式可能反映了潜在疾病生物学的差异。鼓励进一步研究转移部位和组织学亚型之间免疫、分子和遗传特征的差异。