Department of Orthopaedic Surgery, Graduate School of Medical Sciences, Kanazawa University, 13-1, Takaramachi, Kanazawa-city, Ishikawa, 920-8641, Japan.
Department of Pathology, Kanazawa University, Kanazawa, Japan.
Sci Rep. 2021 Jan 21;11(1):1989. doi: 10.1038/s41598-020-80504-w.
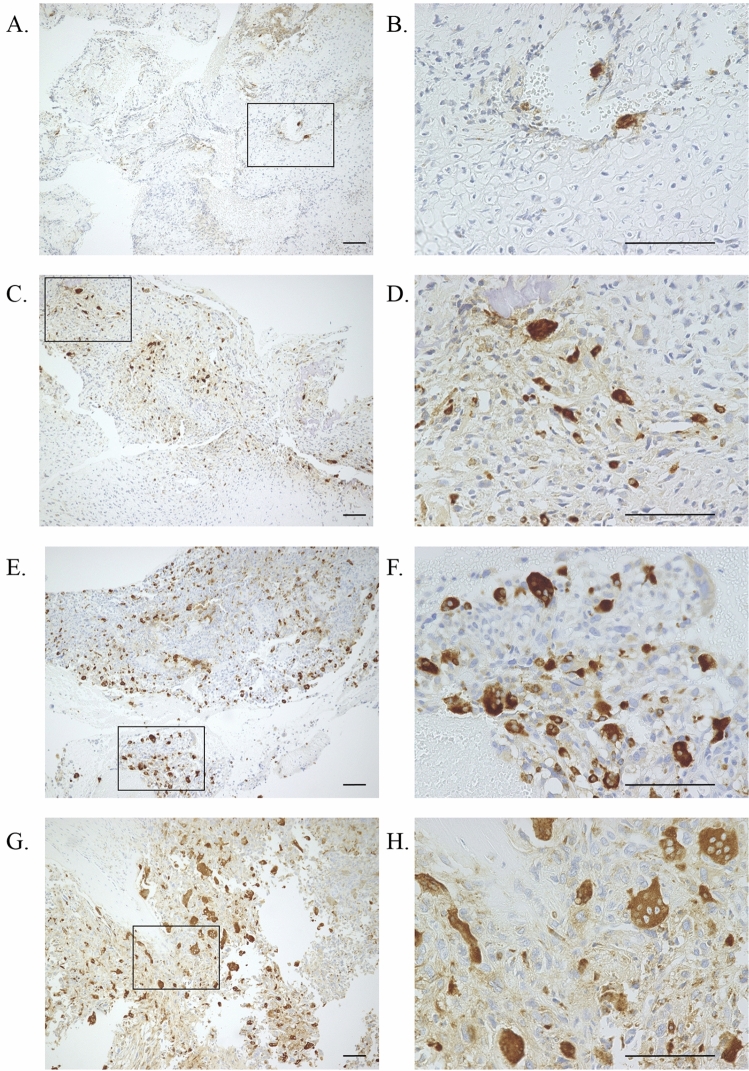
Osteosarcoma is the most common primary malignant bone tumor, and its standard treatment is a combination of surgery and chemotherapy. A poor response to chemotherapy causes unfavorable oncological outcomes. We investigated the correlation between osteoclast differentiation in biopsy specimens and the efficacy of neoadjuvant chemotherapy in resected specimens. Forty-nine patients who underwent neoadjuvant chemotherapy and subsequent surgical treatment at our institution between 1999 and 2018 were enrolled. Using medical records, we investigated the age, sex, tumor size, location, subtype, staging, chemotherapy agents (doxorubicin, cisplatin, ifosfamide, and methotrexate), number of neoadjuvant chemotherapy courses, number of osteoclasts in biopsy specimens, and efficacy of neoadjuvant chemotherapy according to the Rosen and Huvos classification (Grade I-IV) in resected specimens. Univariate and multivariate analyses were performed to identify factors predictive of a good response in resected specimens after neoadjuvant chemotherapy. A good response (Grade III/IV) was detected in 25, while a poor response (Grade I/II) was detected in 24. According to the multivariate analysis, ≥ 46 years old (odds ratio [OR], 0.05; 95% confidence interval [CI], 0.01-0.45; p < 0.01) and ≥ 5 mature osteoclasts in a biopsy specimen (OR, 36.9; 95% CI, 6.03-225; p < 0.01) were significantly associated with the neoadjuvant chemotherapy efficacy. The accuracy for predicting a good response to chemotherapy based on ≥ 5 osteoclasts in a biopsy specimen in patients < 46 years old was 85%. The number of mature osteoclasts in biopsy specimens is a simple factor for predicting the efficacy of chemotherapy before treatment, although further studies will be required to determine the underlying mechanism.
骨肉瘤是最常见的原发性恶性骨肿瘤,其标准治疗方法是手术和化疗相结合。化疗反应不良导致不良的肿瘤学结果。我们研究了活检标本中破骨细胞分化与新辅助化疗后切除标本疗效之间的相关性。1999 年至 2018 年期间,我们机构收治了 49 例接受新辅助化疗和随后手术治疗的患者。通过病历调查,我们根据 Rosen 和 Huvos 分级(I-IV 级)研究了年龄、性别、肿瘤大小、位置、亚型、分期、化疗药物(多柔比星、顺铂、异环磷酰胺和甲氨蝶呤)、新辅助化疗疗程数、活检标本中破骨细胞数和新辅助化疗疗效。进行单因素和多因素分析以确定新辅助化疗后切除标本疗效的预测因素。25 例检测到良好反应(III/IV 级),24 例检测到不良反应(I/II 级)。多因素分析显示,年龄≥46 岁(比值比 [OR],0.05;95%置信区间 [CI],0.01-0.45;p<0.01)和活检标本中≥5 个成熟破骨细胞(OR,36.9;95%CI,6.03-225;p<0.01)与新辅助化疗疗效显著相关。在年龄<46 岁的患者中,基于活检标本中≥5 个成熟破骨细胞预测化疗反应良好的准确率为 85%。活检标本中成熟破骨细胞的数量是预测治疗前化疗疗效的一个简单因素,但需要进一步研究以确定其潜在机制。