Sebastião Yuri V, Metzger Gregory A, Chisolm Deena J, Xiang Henry, Cooper Jennifer N
Center for Surgical Outcomes Research and Center for Innovation in Pediatric Practice, Abigail Wexner Research Institute at Nationwide Children's Hospital, Columbus, OH, USA.
Present address: Division of Global Women's Health, School of Medicine, University of North Carolina, Chapel Hill, NC, USA.
Inj Epidemiol. 2021 Jan 25;8(1):4. doi: 10.1186/s40621-021-00298-x.
We aimed to estimate the impact of the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coding transition on traumatic injury-related hospitalization trends among young adults across a geographically and demographically diverse group of U.S. states.
Interrupted time series analyses were conducted using statewide inpatient databases from 12 states and including traumatic injury-related hospitalizations in adults aged 19-44 years in 2011-2017. Segmented regression models were used to estimate the impact of the October 2015 coding transition on external cause of injury (ECOI) completeness (percentage of hospitalizations with a documented ECOI code) and on population-level rates of injury-related hospitalizations by nature, intent, mechanism, and severity of injury.
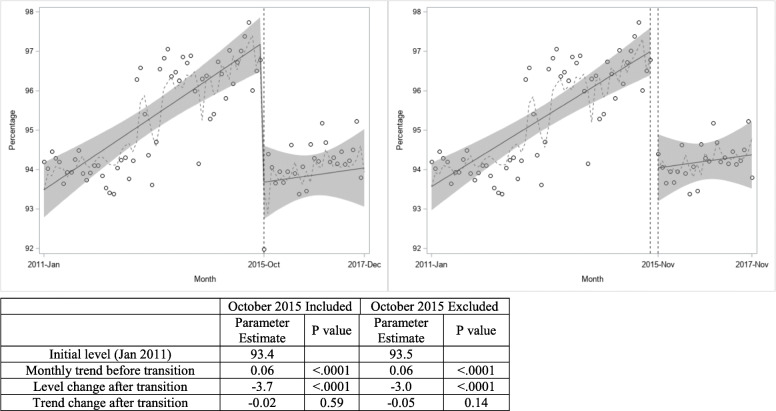
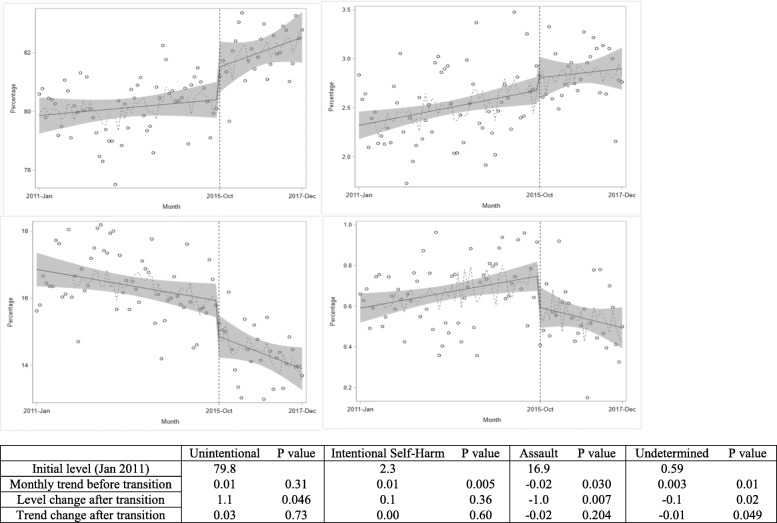
The transition to ICD-10-CM was associated with a drop in ECOI completion in the transition month (- 3.7%; P < .0001), but there was no significant change in the positive trend in ECOI completion from the pre- to post-transition periods. There were significant increases post-transition in the measured rates of hospitalization for traumatic brain injury (TBI), unintentional injury, mild injury (injury severity score (ISS) < 9), and injuries caused by drowning, firearms, machinery, other pedestrian, suffocation, and unspecified mechanism. Conversely, there were significant decreases in October 2015 in the rates of hospitalization for assault, injuries of undetermined intent, injuries of moderate severity (ISS 9-15), and injuries caused by fire/burn, other pedal cyclist, other transportation, natural/environmental, and other specified mechanism. A significant increase in the percentage of hospitalizations classified as resulting from severe injury (ISS > 15) was observed when the general equivalence mapping maximum severity method for converting ICD-10-CM codes to ICD-9-CM codes was used. State-specific results for the outcomes of ECOI completion and TBI-related hospitalization rates are provided in an online supplement.
The U.S. transition from ICD-9-CM to ICD-10-CM coding led to a significant decrease in ECOI completion and several significant changes in measured rates of injury-related hospitalizations by injury intent, mechanism, nature, and severity. The results of this study can inform the design and analysis of future traumatic injury-related health services research studies that use both ICD-9-CM and ICD-10-CM coded data.
II (Interrupted Time Series).
我们旨在评估《国际疾病分类第十次修订本,临床修订版》(ICD - 10 - CM)编码转换对美国不同地理和人口特征的各州年轻成年人创伤性损伤相关住院趋势的影响。
使用来自12个州的全州住院患者数据库进行中断时间序列分析,纳入2011 - 2017年19 - 44岁成年人的创伤性损伤相关住院病例。采用分段回归模型来评估2015年10月编码转换对损伤外部原因(ECOI)完整性(有记录的ECOI编码的住院病例百分比)以及按损伤性质、意图、机制和严重程度划分的人群层面损伤相关住院率的影响。
向ICD - 10 - CM的转换与转换月ECOI完整性的下降相关(-3.7%;P <.0001),但从转换前到转换后的时期,ECOI完整性的正向趋势没有显著变化。转换后,创伤性脑损伤(TBI)、意外伤害、轻度损伤(损伤严重程度评分(ISS)<9)以及溺水、火器、机械、其他行人、窒息和未明确机制导致的损伤的住院率显著增加。相反,2015年10月,袭击、意图不明的损伤、中度损伤(ISS 9 - 15)以及火灾/烧伤、其他骑自行车者、其他交通、自然/环境和其他特定机制导致的损伤的住院率显著下降。当使用将ICD - 10 - CM编码转换为ICD - 9 - CM编码的一般等效映射最大严重程度方法时,观察到归类为严重损伤(ISS>15)导致的住院病例百分比显著增加。ECOI完整性和TBI相关住院率结果的各州特定结果在在线补充资料中提供。
美国从ICD - 9 - CM编码向ICD - 10 - CM编码的转换导致ECOI完整性显著下降,并使按损伤意图、机制、性质和严重程度划分的损伤相关住院率出现了一些显著变化。本研究结果可为未来使用ICD - 9 - CM和ICD - 10 - CM编码数据的创伤性损伤相关卫生服务研究的设计和分析提供参考。
II(中断时间序列)。