Institute of Psychiatry, Psychology & Neuroscience, King's College London, London UK.
Centre for Health Services Studies, University of Kent, Canterbury, UK.
Int J Drug Policy. 2021 Jul;93:103113. doi: 10.1016/j.drugpo.2021.103113. Epub 2021 Jan 22.
Alcohol consumption and related harm increase rapidly from the age of 12 years. We evaluated whether alcohol screening and brief intervention is effective and cost-effective in delaying hazardous or harmful drinking amongst low-risk or abstaining adolescents attending Emergency Departments (EDs).
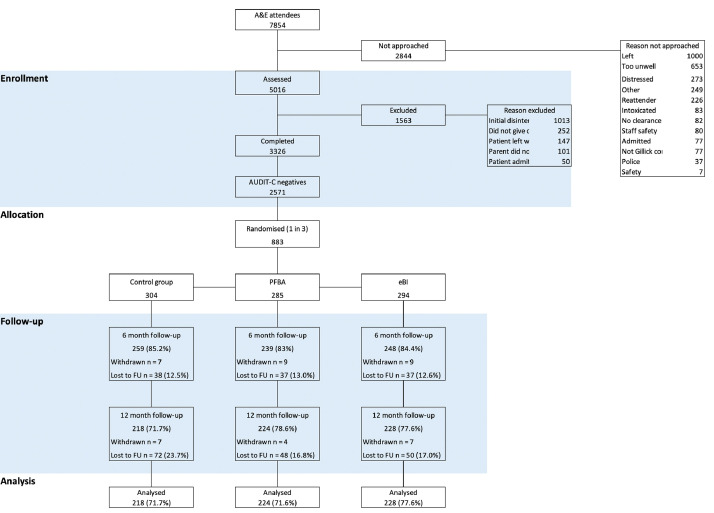
This ten-centre, three-arm, parallel-group, single-blind, pragmatic, individually randomised trial screened ED attenders aged between 14 and 17 years for alcohol consumption. We sampled at random one third of those scoring at most 2 on AUDIT-C who had access to the internet and, if aged under 16, were Gillick competent or had informed consent from parent or guardian. We randomised them between: screening only (control intervention); one session of face-to-face Personalised Feedback and Brief Advice (PFBA); and PFBA plus an electronic brief intervention (eBI) on smartphone or web. We conducted follow-up after six and 12 months. The principal outcomes were alcohol consumed over the 3 months before 12-month follow up, measured by AUDIT-C; and quality-adjusted life-years.
Between October 2014 and May 2015, we approached 5,016 eligible patients of whom 3,326 consented to be screened and participate in the trial; 2,571 of these were low-risk drinkers or abstainers, consuming an average 0.14 units per week. We randomised: 304 to screening only; 285 to PFBA; and 294 to PFBA and eBI. We found no significant difference between groups, notably in weekly alcohol consumption: those receiving screening only drank 0.10 units (95% confidence interval 0.05 to 0.18); PFBA 0.12 (0.06 to 0.21); PFBA and eBI 0.10 (0.05 to 0.19).
While drinking levels remained low in this population, this trial found no evidence that PFBA with or without eBI was more effective than screening alone in reducing or delaying alcohol consumption.
酒精消费及其相关危害在 12 岁时迅速增加。我们评估了在急诊科(ED)就诊的低风险或不饮酒的青少年中,酒精筛查和简短干预是否能有效且具有成本效益,以延缓危险或有害饮酒。
这是一项十中心、三臂、平行组、单盲、实用、个体随机试验,对年龄在 14 至 17 岁之间的 ED 就诊者进行酒精消费筛查。我们随机抽取 AUDIT-C 得分最高为 2 的三分之一,且有上网条件的青少年,如果年龄在 16 岁以下,具有 Gillick 能力或得到父母或监护人的知情同意。我们将他们随机分配到以下三组:仅筛查(对照组);面对面个性化反馈和简短建议(PFBA);以及 PFBA 加智能手机或网络上的电子简短干预(eBI)。我们在 6 个月和 12 个月后进行随访。主要结局是在 12 个月随访前的 3 个月内消耗的酒精量,通过 AUDIT-C 测量;以及质量调整生命年。
2014 年 10 月至 2015 年 5 月,我们共接触了 5016 名符合条件的患者,其中 3326 名同意接受筛查并参加试验;其中 2571 名是低风险饮酒者或不饮酒者,平均每周饮酒 0.14 单位。我们随机分配:304 名仅接受筛查;285 名接受 PFBA;294 名接受 PFBA 和 eBI。我们没有发现组间的显著差异,特别是在每周饮酒量方面:仅接受筛查的组饮用 0.10 单位(95%置信区间 0.05 至 0.18);接受 PFBA 的组饮用 0.12 单位(0.06 至 0.21);接受 PFBA 和 eBI 的组饮用 0.10 单位(0.05 至 0.19)。
虽然在这个人群中饮酒水平仍然较低,但这项试验没有发现 PFBA 加或不加 eBI 比单独筛查更能有效减少或延缓饮酒的证据。