Feng Wen, Li Yuan, Shen Lei, Zhang Qin, Cai Xu-Wei, Zhu Zheng-Fei, Sun Meng-Hong, Chen Hai-Quan, Fu Xiao-Long
Department of Radiation Oncology, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, China.
Department of Pathology, Fudan University Shanghai Cancer Center, Shanghai, China.
Ther Adv Med Oncol. 2021 Jan 11;13:1758835920984975. doi: 10.1177/1758835920984975. eCollection 2021.
Completely resected stage IIIA(N2) non-small cell lung cancer (NSCLC) comprises a heterogeneous population according to discrepancies in survival prognosis. Accumulating evidence suggests that tumor-infiltrating lymphocytes (TILs) are clinically significant, despite a lack of consensus regarding the immunoscore (IS) in NSCLC. Here, we determined the prognostic value of the immune microenvironment as an IS in a uniform cohort of patients with completely resected stage IIIA(N2) NSCLC.
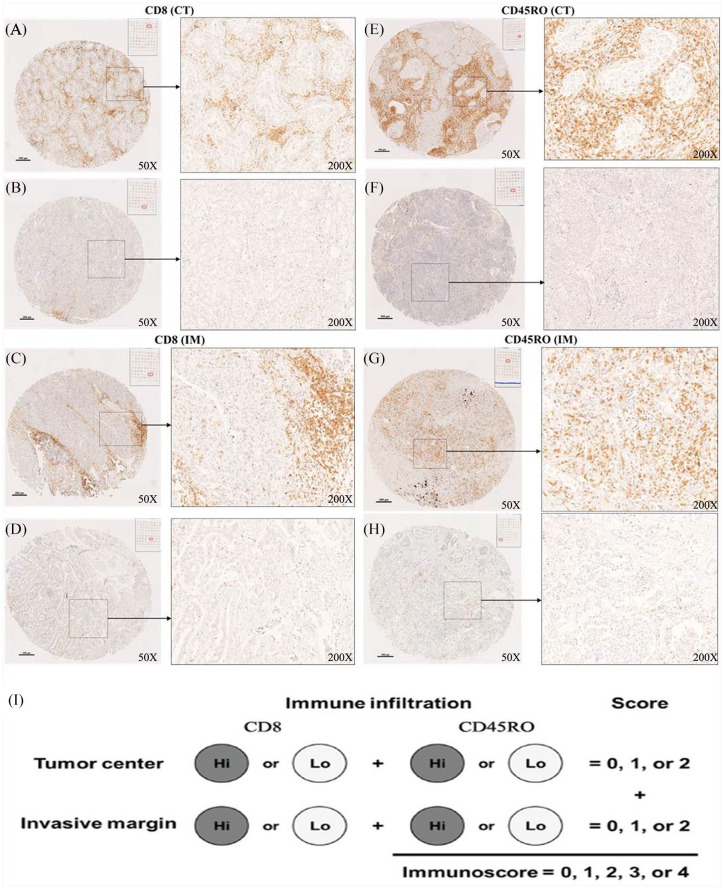
Consecutive patients with pathologically confirmed stage IIIA(N2) NSCLC and who underwent complete resection (2005-2012) were retrospectively reviewed. Tissue microarrays (TMAs) were constructed from surgical paraffin-embedded primary lung tumor specimen. For each case, two representative regions from the tumor center (CT) and two from the invasive margin (IM) containing the highest density of lymphocytes were selected. Densities of CD3+, CD45RO+, and CD8+ lymphocytes were assessed using immunohistochemistry (IHC) by specialized pathologists according to predefined scoring scales. Patients were classified according to IS definition based on TIL type, density, and distribution, and relationships between IS and prognosis were evaluated.
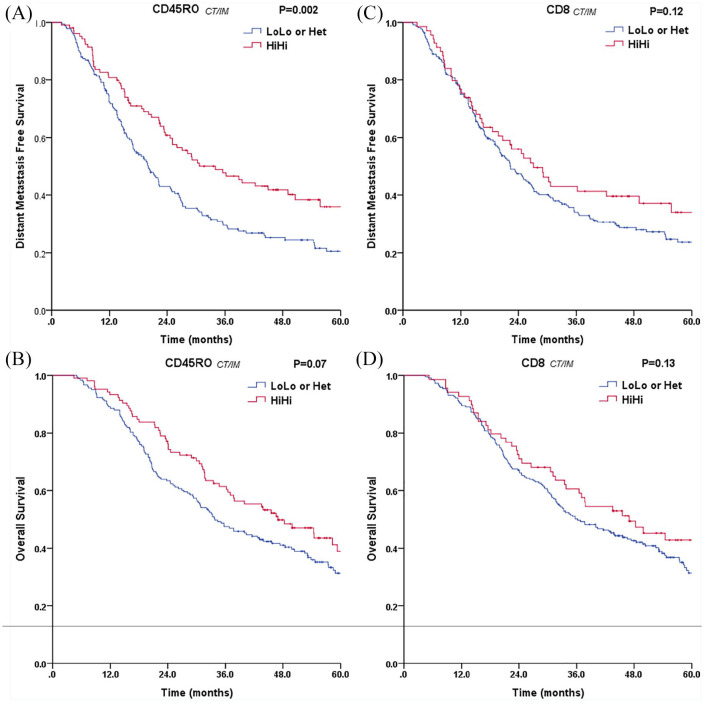
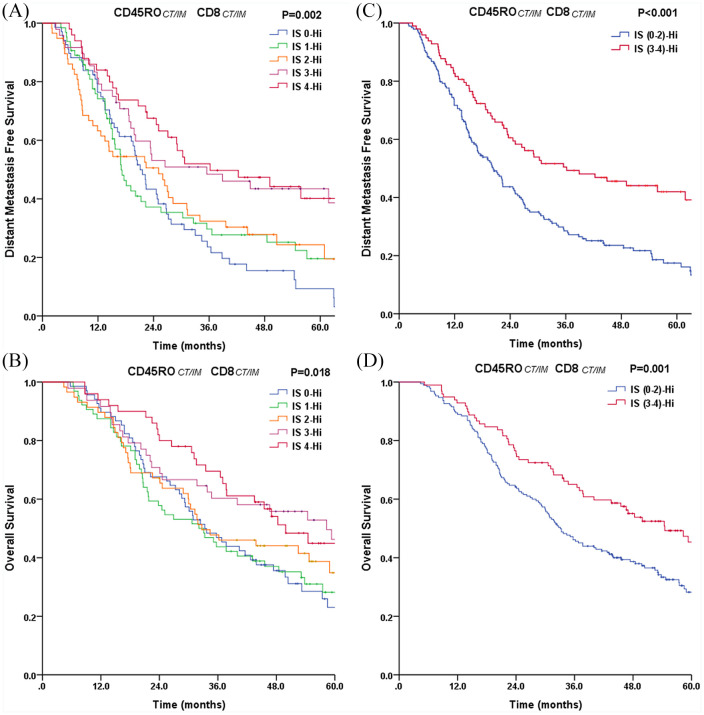
Patients ( = 288) with complete IHC-based TMA spots were included. Univariate analyses showed that CD3+ T cell density was associated with neither overall survival (OS) nor distant metastasis-free survival (DMFS), whereas CD45RO+ T cell density in the IM was a significant prognostic factor for DMFS ( = 0.02) and was predictive of OS ( = 0.05). Combined CD45RO+ and CD8+ cell infiltration in tumor regions (CT and IM) significantly improved IS prognostic impact. Multivariate analyses revealed IS as an independent prognostic predictor for both DMFS ( = 0.001) and OS ( = 0.002).
The proposed IS might provide valuable prognostic information, including prediction of DMFS and OS in stage IIIA(N2) NSCLC patients. Larger patient cohorts are needed to validate this IS classification, which might assist with accurate risk stratification and treatment decisions.
完全切除的IIIA期(N2)非小细胞肺癌(NSCLC)患者群体的生存预后存在差异,具有异质性。越来越多的证据表明,肿瘤浸润淋巴细胞(TILs)具有临床意义,尽管对于NSCLC的免疫评分(IS)尚未达成共识。在此,我们在一组完全切除的IIIA期(N2)NSCLC患者中,确定了免疫微环境作为IS的预后价值。
回顾性分析2005年至2012年期间连续收治的、经病理证实为IIIA期(N2)NSCLC且接受了完全切除的患者。组织微阵列(TMA)由手术石蜡包埋的原发性肺肿瘤标本构建而成。对于每个病例,从肿瘤中心(CT)选取两个具有代表性的区域,从浸润边缘(IM)选取两个淋巴细胞密度最高的区域。由专业病理学家根据预定义的评分标准,采用免疫组织化学(IHC)方法评估CD3 +、CD45RO +和CD8 +淋巴细胞的密度。根据基于TIL类型、密度和分布的IS定义对患者进行分类,并评估IS与预后之间的关系。
纳入了基于IHC的TMA斑点完整的288例患者。单因素分析显示,CD3 + T细胞密度与总生存期(OS)和无远处转移生存期(DMFS)均无关,而IM中CD45RO + T细胞密度是DMFS的显著预后因素(P = 0.02),且可预测OS(P = 0.05)。肿瘤区域(CT和IM)中CD45RO +和CD8 +细胞的联合浸润显著提高了IS的预后影响。多因素分析显示,IS是DMFS(P = 0.001)和OS(P = 0.002)的独立预后预测指标。
所提出的IS可能提供有价值的预后信息,包括预测IIIA期(N2)NSCLC患者的DMFS和OS。需要更大规模的患者队列来验证这种IS分类,这可能有助于准确的风险分层和治疗决策。