Ye Jiru, Zhang Xiaoqing, Zhu Feng, Tang Yao
Department of Respiratory and Critical Care Medicine, The Third Affiliated Hospital of Soochow University, Changzhou, Jiangsu 213003, P.R. China.
Department of Respiratory and Critical Care Medicine, Wuxi Fifth People's Hospital, Wuxi, Jiangsu 214000, P.R. China.
Exp Ther Med. 2021 Mar;21(3):182. doi: 10.3892/etm.2021.9613. Epub 2021 Jan 5.
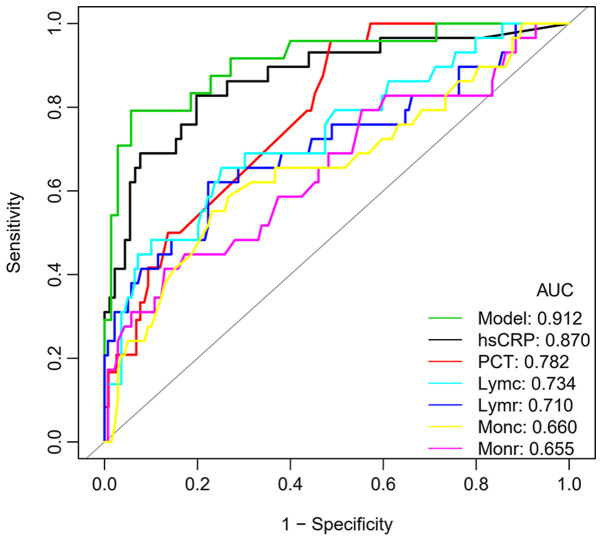
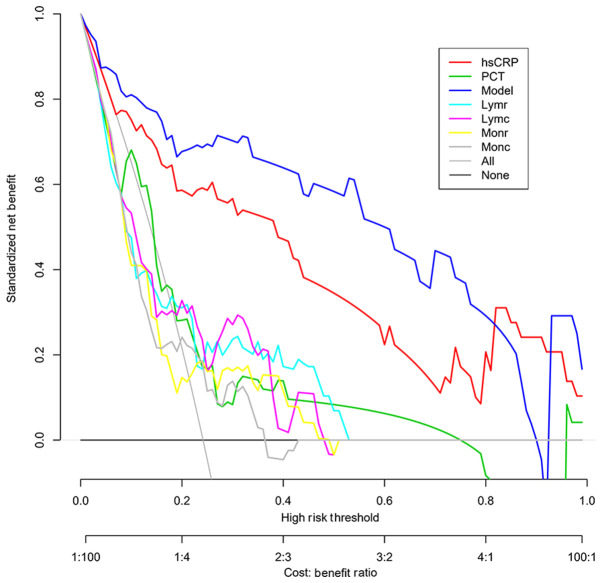
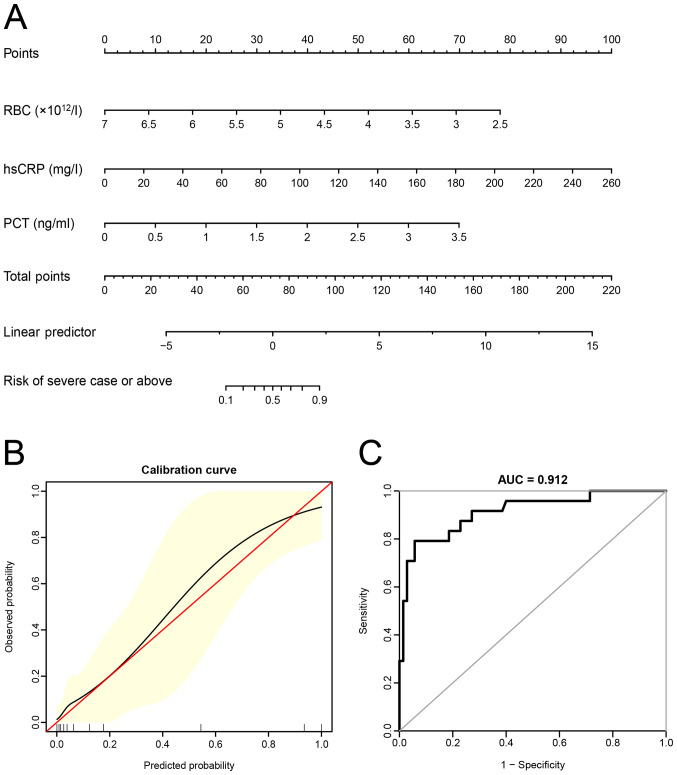
In the present study, a prediction model with combined laboratory indexes in risk stratification of patients with COVID-19 was established and tested. The data of 170 patients with COVID-19 who were divided into an asymptomatic-moderate group (141 cases) and severe or above group (29 cases) were retrospectively analyzed. The clinical characteristics and laboratory indexes of the two groups were compared. Multivariate logistic regression analysis was performed to construct the prediction model based on laboratory indexes. A receiver operating characteristic (ROC) curve analysis was used to compare the diagnostic efficacy of different indexes. Decision curve analysis (DCA) was performed to quantify and compare the clinical validity of the prediction models. There were significant differences in blood cell count, high-sensitivity C-reactive protein (hsCRP) and procalcitonin (PCT) levels between the severe or above group and the asymptomatic-moderate group (all P<0.05). Among all individual indexes, hsCRP had the highest diagnostic efficacy (area under the curve=0.870), with a sensitivity and specificity of 0.828 and 0.802, respectively. The red blood cell count, hsCRP and PCT were used to construct the prediction model. The AUC of the prediction model was higher than that of hsCRP (0.912 vs. 0.870) but the difference was not significant (P=0.307). DCA suggested that the net benefit of the prediction model was higher than that of hsCRP in most cases and significantly higher than that of PCT, lymphocytes and monocytes. The prediction model with combined laboratory indexes was able to more effectively predict the clinical classification of patients with COVID-19 and may be used as a tool for risk stratification of patients.
在本研究中,建立并测试了一个用于新型冠状病毒肺炎(COVID-19)患者风险分层的联合实验室指标预测模型。对170例COVID-19患者的数据进行回顾性分析,这些患者被分为无症状-中度组(141例)和重度及以上组(29例)。比较了两组的临床特征和实验室指标。基于实验室指标进行多因素逻辑回归分析以构建预测模型。采用受试者工作特征(ROC)曲线分析比较不同指标的诊断效能。进行决策曲线分析(DCA)以量化和比较预测模型的临床有效性。重度及以上组与无症状-中度组之间的血细胞计数、高敏C反应蛋白(hsCRP)和降钙素原(PCT)水平存在显著差异(均P<0.05)。在所有单项指标中,hsCRP的诊断效能最高(曲线下面积=0.870),敏感性和特异性分别为0.828和0.802。采用红细胞计数、hsCRP和PCT构建预测模型。预测模型的AUC高于hsCRP(0.912对0.870),但差异无统计学意义(P=0.307)。DCA表明,在大多数情况下,预测模型的净效益高于hsCRP,且显著高于PCT、淋巴细胞和单核细胞。联合实验室指标的预测模型能够更有效地预测COVID-19患者的临床分类,可作为患者风险分层的工具。