Price Robert A, Jin Lihui, Meyer Joshua, Chen Lili, Lin Teh, Eldib Ahmed, Chen Xiaoming, Liu Jie, Veltchev Iavor, Wang Lu, Ma Charlie
Department of Radiation Oncology, Fox Chase Cancer Center, Philadelphia, Pennsylvania.
Adv Radiat Oncol. 2020 Oct 14;6(1):100594. doi: 10.1016/j.adro.2020.09.027. eCollection 2021 Jan-Feb.
The purpose of this work is to present a practical, structured process allowing for consistent, safe radiation therapy delivery in the re-treatment environment.
A process for reirradiation is described with documentation in the form of a special physics consultation. Data acquisition associated with previous treatment is described from highest to lowest quality. Methods are presented for conversion to equieffective dose, as well as our departmental assumptions for tissue repair. The generation of organ-at-risk available physical dose for use in treatment planning is discussed. Results using our methods are compared with published values after conversion to biologically effective dose. Utilization of pulsed-low-dose-rate delivery is described, and data for reirradiation using these methods over the previous 5 years are presented.
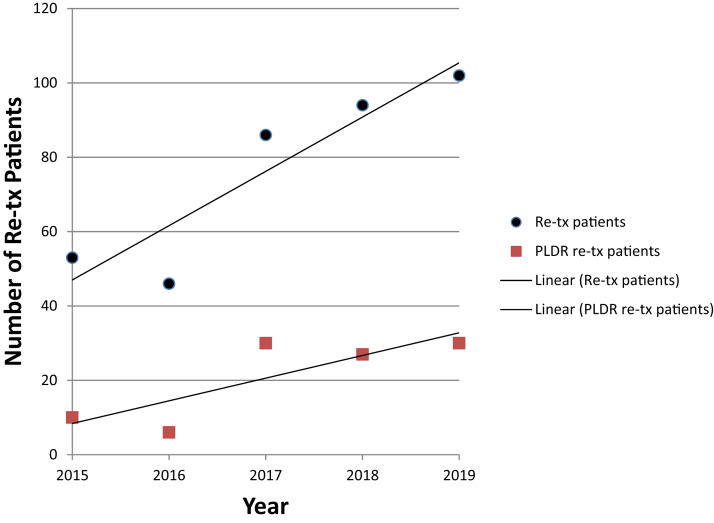
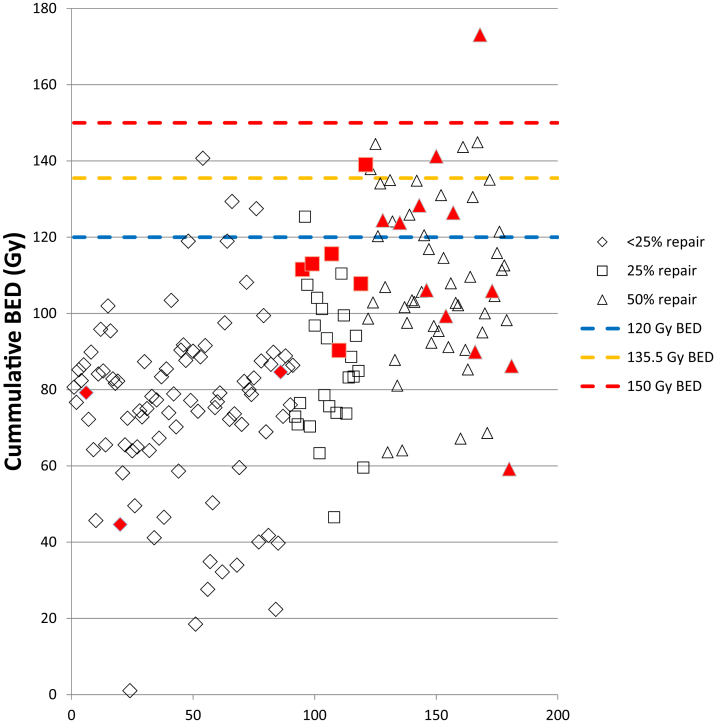
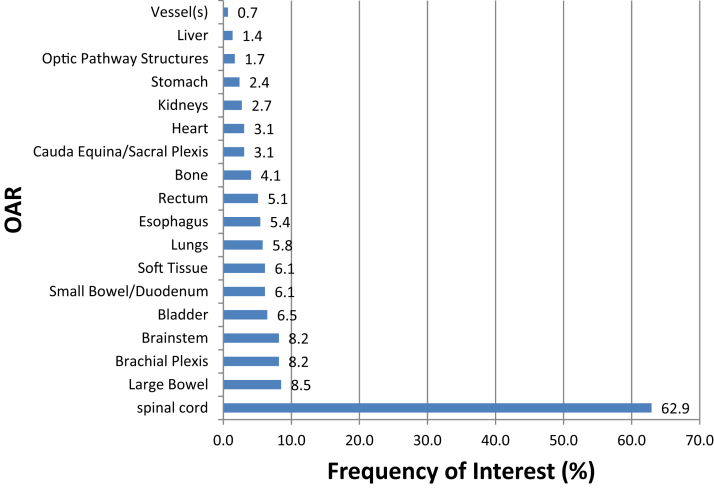
Between 2015 and 2019, the number of patients in our department requiring equieffective dose calculation has doubled. We have developed guidelines for estimation of sublethal damage repair as a function of time between treatment courses ranging from 0% for <6 months to 50% for >1 year. These guidelines were developed based on available spinal cord data because we found that 84% of organs at risk involved nerve-like tissues. The average percent repair used increased from 32% to 37% over this time period. When comparing the results obtained using our methods with published values, 99% of patients had a cumulative biologically effective dose below the limits established for acceptable myelopathy rates. Pulsed-low-dose-rate use over this period tripled with an average prescription dose of 49 Gy.
The methods described result in safe, effective treatment in the reirradiation setting. Further correlation with patient outcomes and side effects is warranted.
本研究旨在提出一种实用、结构化的流程,以便在再治疗环境中实现一致、安全的放射治疗。
描述了一种再照射流程,并以特殊物理会诊的形式进行记录。从最高质量到最低质量描述了与先前治疗相关的数据采集。介绍了转换为等效剂量的方法以及我们科室关于组织修复的假设。讨论了用于治疗计划的危及器官可用物理剂量的生成。将使用我们方法得到的结果转换为生物等效剂量后与已发表的值进行比较。描述了脉冲低剂量率照射的应用,并给出了过去5年使用这些方法进行再照射的数据。
2015年至2019年期间,我们科室需要计算等效剂量的患者数量增加了一倍。我们制定了亚致死性损伤修复估计指南,该指南是治疗疗程间隔时间的函数,间隔时间小于6个月时为0%,大于1年时为50%。这些指南是根据现有的脊髓数据制定的,因为我们发现84%的危及器官涉及神经样组织。在此期间,平均使用的修复百分比从32%增加到37%。将使用我们方法得到的结果与已发表的值进行比较时,99%的患者累积生物等效剂量低于为可接受的脊髓病发生率设定的限值。在此期间,脉冲低剂量率照射的使用增加了两倍,平均处方剂量为49 Gy。
所描述的方法在再照射环境中可实现安全、有效的治疗。有必要进一步将其与患者预后和副作用进行关联研究。