Division of Gastroenterology and Hepatology, Graduate School of Medical and Dental Sciences, Niigata University, Niigata, Japan.
Costello Medical, Boston, MA, USA.
J Gastroenterol. 2021 Mar;56(3):274-284. doi: 10.1007/s00535-021-01759-2. Epub 2021 Jan 26.
This study examined demographics, comorbidities and healthcare resource use (HCRU) and costs among Japanese patients with nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH).
We conducted a repeated cross-sectional analysis of the Medical Data Vision (MDV) claims database, from January 2011 to March 2018. Demographics were described at index date and by calendar year; a "NASH" subpopulation included patients with ≥ 1 claim for NASH at any time. Prevalence of pre-specified comorbidities of interest and data-emergent top comorbidities were estimated. All-cause HCRU and costs were quantified by calendar year. Outcomes were compared between 2011 and 2017 using partially overlapping t tests.
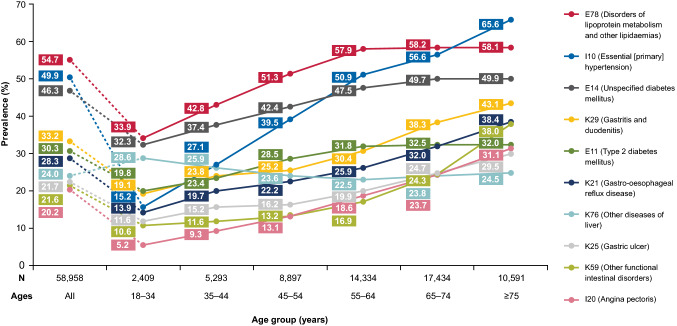
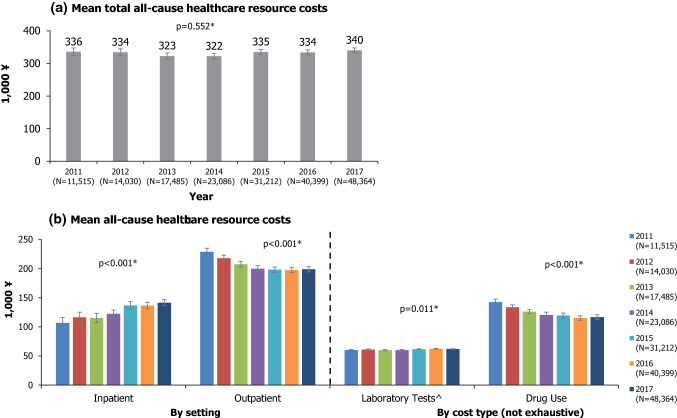
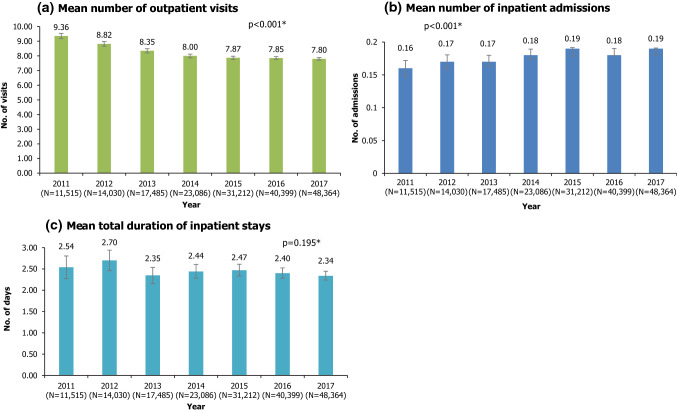
58,958 patients (mean age 61.6 years; 55.5% male) were included. 1139 patients (2%) were in the NASH subpopulation. At baseline, comorbid cardiovascular disease (69.4%), diabetes (62.1%) and hyperlipidaemia (54.4%) were most prevalent; comorbidity prevalence increased with age. Mean outpatient visits decreased from 9.36 per patient in 2011 to 7.80 in 2017; mean inpatient admissions increased (both p < 0.001 for 2011 vs 2017). Mean total all-cause healthcare costs ranged from ¥322,206 to ¥340,399 per patient per year between 2011 and 2017. Although total all-cause healthcare costs did not change significantly (p = 0.552), cost burden shifted from the outpatient to inpatient setting between 2011 and 2017. All-cause healthcare resource use/costs were generally higher for the NASH subgroup compared with the overall population.
There is a high burden of disease among Japanese NAFLD/NASH patients, including a high prevalence of comorbidities which generally increase with age. Accordingly, substantial all-cause HCRU and costs were incurred.
本研究调查了日本非酒精性脂肪性肝病(NAFLD)和非酒精性脂肪性肝炎(NASH)患者的人口统计学、合并症和医疗资源使用(HCRU)及费用情况。
我们对 2011 年 1 月至 2018 年 3 月的医疗数据视觉(MDV)索赔数据库进行了重复的横断面分析。在索引日期和日历年度描述了人口统计学特征;“NASH”亚组包括任何时候至少有 1 次 NASH 索赔的患者。估计了预先指定的感兴趣的合并症的患病率和数据出现的最高合并症。按日历年度量化了所有原因的 HCRU 和费用。使用部分重叠的 t 检验比较了 2011 年和 2017 年的结果。
共纳入 58958 例患者(平均年龄 61.6 岁;55.5%为男性)。1139 例(2%)患者为 NASH 亚组。基线时,最常见的合并症为心血管疾病(69.4%)、糖尿病(62.1%)和高脂血症(54.4%);合并症的患病率随年龄增长而增加。2011 年每位患者的门诊就诊次数从 9.36 次降至 2017 年的 7.80 次;住院人数增加(2011 年与 2017 年相比,均 p<0.001)。2011 年至 2017 年,每位患者每年的所有原因总医疗费用范围为 322206 日元至 340399 日元。尽管总所有原因医疗费用没有显著变化(p=0.552),但 2011 年至 2017 年,费用负担从门诊转移到了住院治疗。与总体人群相比,NASH 亚组的所有原因医疗资源使用/费用通常更高。
日本 NAFLD/NASH 患者的疾病负担较高,包括普遍随年龄增长而增加的合并症高发率。因此,发生了大量的全因 HCRU 和费用。