Rheumatology, CHU Montpellier, Montpellier, France
Altoona Center for Clinical Research, Duncansville, Pennsylvania, USA.
Ann Rheum Dis. 2021 Jul;80(7):848-858. doi: 10.1136/annrheumdis-2020-219214. Epub 2021 Jan 27.
To evaluate the efficacy and safety of the Janus kinase-1-preferential inhibitor filgotinib versus placebo or tumour necrosis factor-α inhibitor therapy in patients with active rheumatoid arthritis (RA) despite ongoing treatment with methotrexate (MTX).
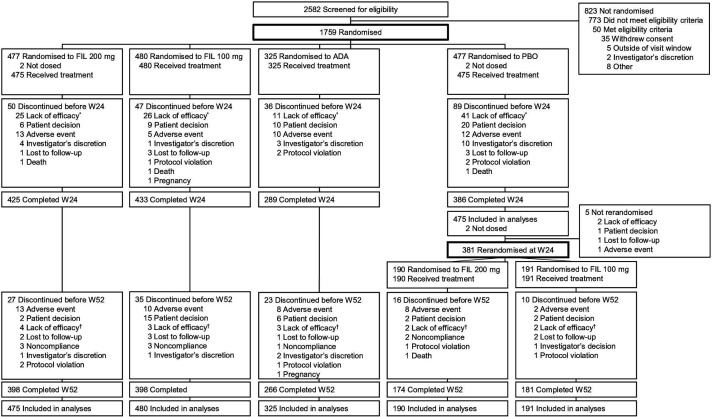
This 52-week, multicentre, double-blind, placebo-controlled and active-controlled phase III trial evaluated once-daily oral filgotinib in patients with RA randomised 3:3:2:3 to filgotinib 200 mg (FIL200) or filgotinib 100 mg (FIL100), subcutaneous adalimumab 40 mg biweekly, or placebo (through week 24), all with stable weekly background MTX. The primary endpoint was the proportion of patients achieving 20% improvement in American College of Rheumatology criteria (ACR20) at week 12. Additional efficacy outcomes were assessed sequentially. Safety was assessed from adverse events and laboratory abnormalities.
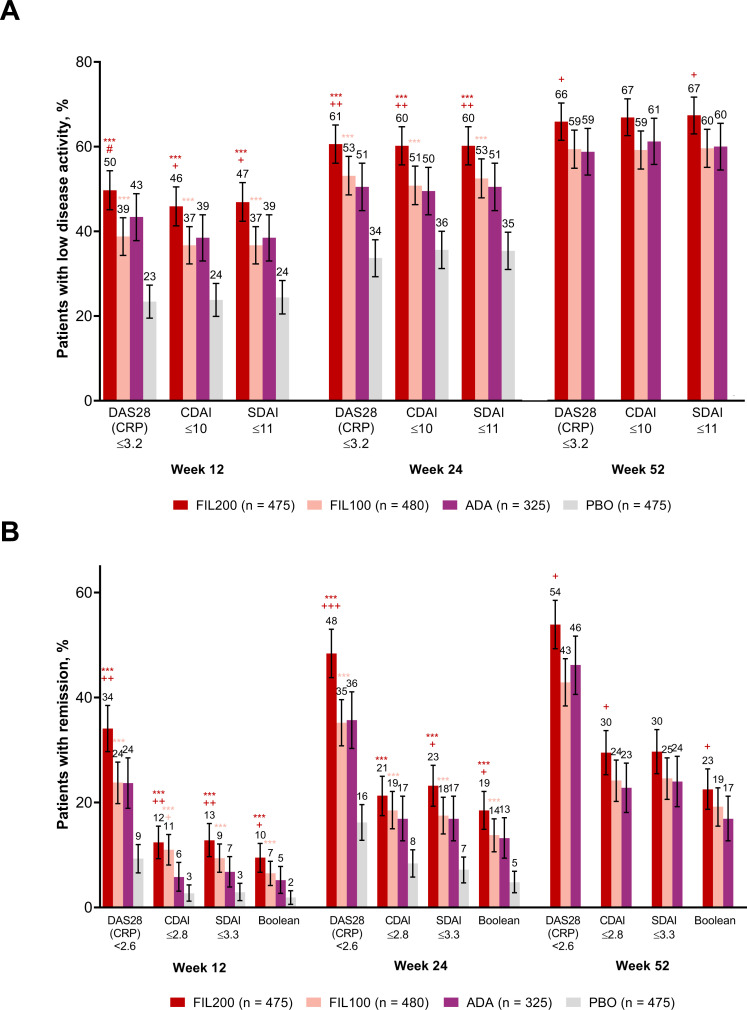
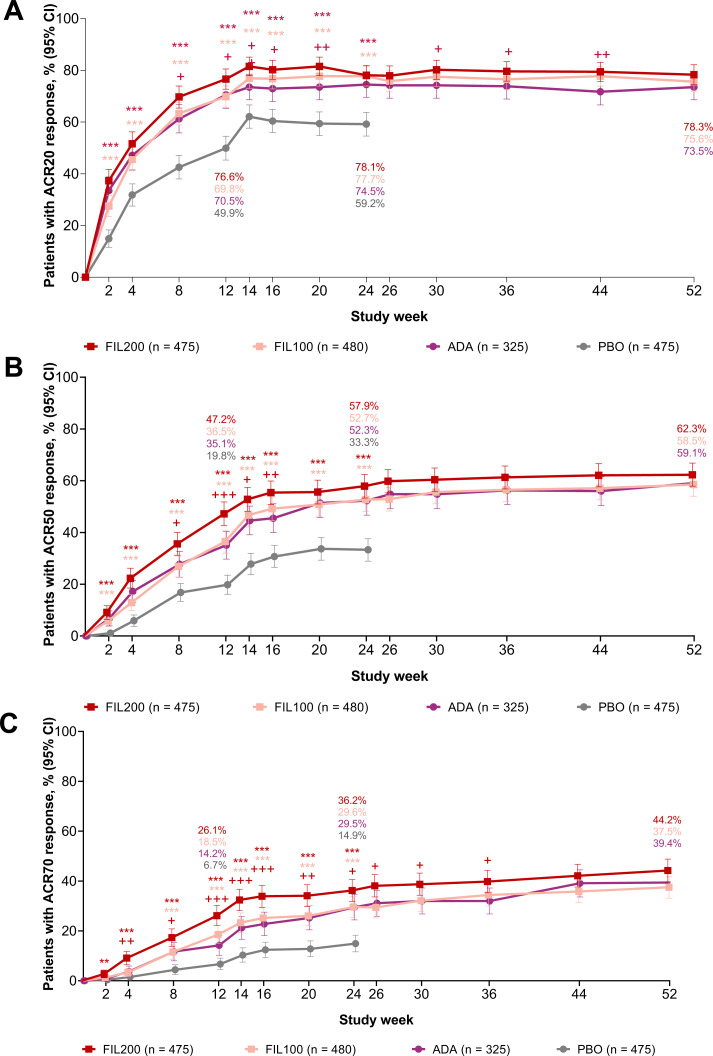
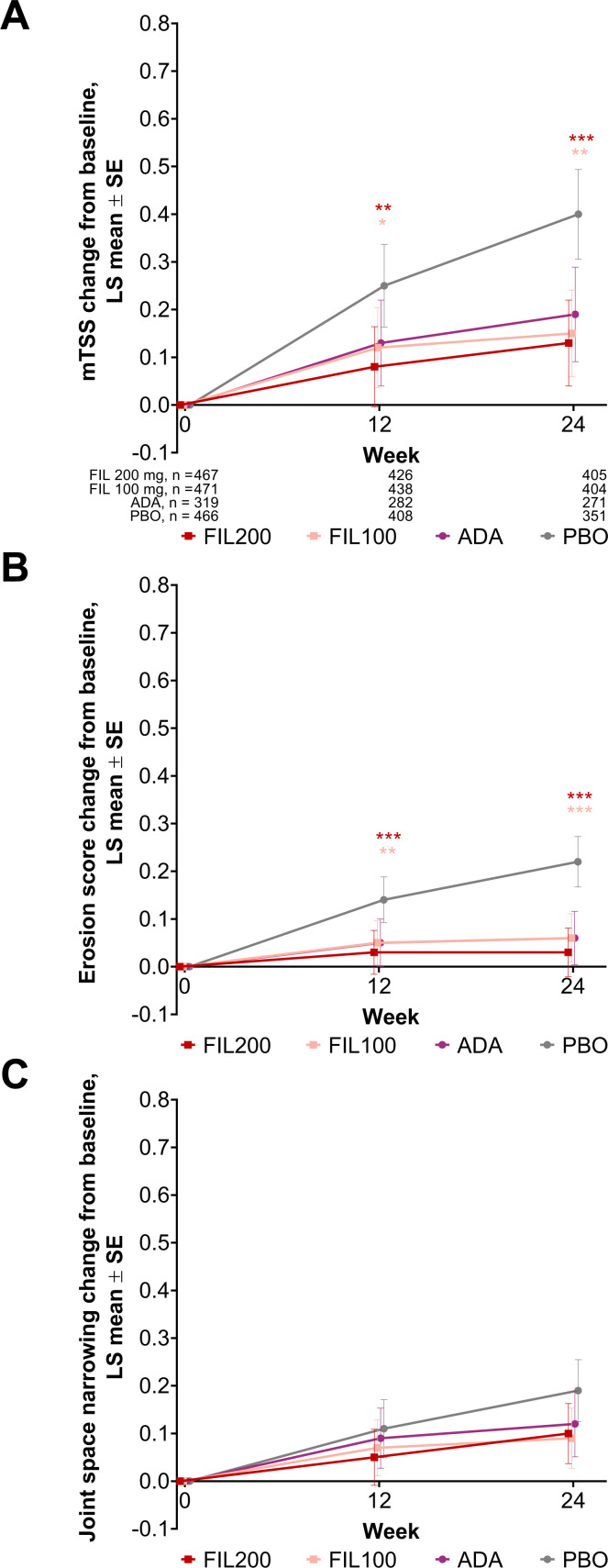
The proportion of patients (n=1755 randomised and treated) achieving ACR20 at week 12 was significantly higher for FIL200 (76.6%) and FIL100 (69.8%) versus placebo (49.9%; treatment difference (95% CI), 26.7% (20.6% to 32.8%) and 19.9% (13.6% to 26.2%), respectively; both p<0.001). Filgotinib was superior to placebo in key secondary endpoints assessing RA signs and symptoms, physical function and structural damage. FIL200 was non-inferior to adalimumab in terms of Disease Activity Score in 28 joints with C reactive protein ≤3.2 at week 12 (p<0.001); FIL100 did not achieve non-inferiority. Adverse events and laboratory abnormalities were comparable among active treatment arms.
Filgotinib improved RA signs and symptoms, improved physical function, inhibited radiographic progression and was well tolerated in patients with RA with inadequate response to MTX. FIL200 was non-inferior to adalimumab.
NCT02889796.
评估 Janus 激酶-1 选择性抑制剂 filgotinib 相较于安慰剂或肿瘤坏死因子-α抑制剂治疗在甲氨蝶呤(MTX)治疗下仍处于活动期的类风湿关节炎(RA)患者中的疗效和安全性。
这是一项为期 52 周、多中心、双盲、安慰剂对照和活性药物对照的 III 期临床试验,评估了每日一次口服 filgotinib 在随机分为 3:3:2:3 组的 RA 患者中的疗效,分别接受 filgotinib 200mg(FIL200)或 100mg(FIL100)、皮下阿达木单抗 40mg 每两周一次、或安慰剂(至第 24 周)治疗,所有患者均接受稳定的每周背景 MTX 治疗。主要终点为第 12 周时达到美国风湿病学会(ACR)20%改善的患者比例(ACR20)。进一步评估了其他疗效终点。从不良事件和实验室异常情况评估安全性。
在第 12 周时,FIL200(76.6%)和 FIL100(69.8%)组达到 ACR20 的患者比例显著高于安慰剂组(49.9%;治疗差异[95%CI],26.7%(20.6%至 32.8%)和 19.9%(13.6%至 26.2%);均 p<0.001)。在评估 RA 体征和症状、身体功能和结构损伤的关键次要终点方面,filgotinib 优于安慰剂。在第 12 周时,与阿达木单抗相比,FIL200 达到了 28 个关节疾病活动度评分(DAS28)且 C 反应蛋白≤3.2 的非劣效性(p<0.001);但 FIL100 未达到非劣效性。在活性治疗组中,不良事件和实验室异常情况相似。
Filgotinib 改善了 RA 体征和症状,改善了身体功能,抑制了影像学进展,并且在对 MTX 反应不足的 RA 患者中具有良好的耐受性。FIL200 与阿达木单抗相当。
NCT02889796。