Department of Radiation Oncology, Henry Ford Cancer Institute, Detroit, Michigan, USA.
Department of Clinical Oncology, Faculty of Medicine, Alexandria University, Egypt.
Asian Pac J Cancer Prev. 2021 Jan 1;22(1):61-68. doi: 10.31557/APJCP.2021.22.1.61.
To compare radiotherapy-induced toxicity for localized prostate-cancer (PCa) treated with versus without daily image-guidance.
We identified consecutive intermediate and high-risk localized PCa patients treated with definitive radiotherapy using intensity-modulated radiotherapy (IMRT) with variable duration of androgen-deprivation therapy (ADT) within 2015-2016 (Arm-A) and 2005-2007 (Arm-B). Arm-A cases received daily online imaging guidance (IGRT) using cone-beam computed tomography (CBCT) unlike Arm-B candidates with no daily IGRT. After reporting demographic, clinico-pathological features and treatment details, we compared acute (within 3 months post-therapy) and late RT-induced toxicities between study groups graded by RTOG/CTCAE criteria. Uni/multivariate analyses (UVA/MVA) were performed to identify independent predictors for RT-related side-effects.
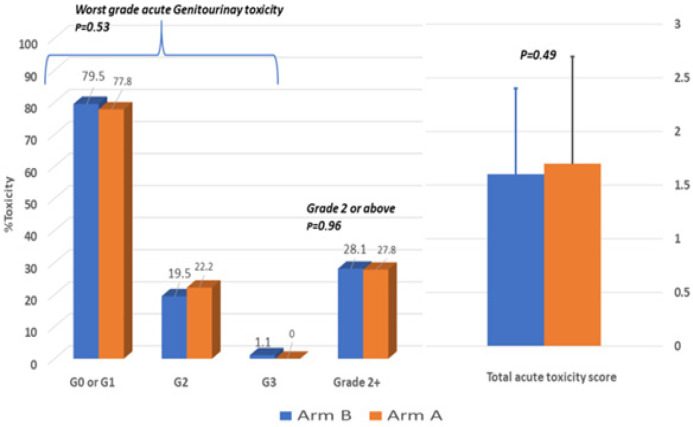
We were able to identify 257 cases who met our inclusion criteria. Overall, median age was 73 years (48-85), 67% had intermediate-risk and 47% received ADT. Arm-A included 72 patients who received IMRT delivered using volumetric-modulated arc therapy (VMAT), whereas, Arm-B was formed of 185 cases who utilized step-and-shoot static IMRT. Clinico-pathological features and treatment details were non-different across study arms except that Arm-A had more Grade Group 3, higher median total dose (79.2 vs. 74 Gy) and more pelvic lymph-nodes RT (p <0.05). Although acute toxicity was similar across groups, Arm-B encountered higher late toxicity score, more intense late genitourinary side-effects (P=0.008), with non-different late lower-gastrointestinal toxicities. On MVA, lack of daily CBCT, African-American race and higher comorbidities were independently predictive for late toxicities. Conclusion: IMRT with daily CBCT permitted safe delivery of dose-escalated IMRT with improved toxicity profile for higher-risk prostate cancer.
比较局部前列腺癌(PCa)接受有和无每日图像引导放疗的放疗诱导毒性。
我们在 2015-2016 年(A 组)和 2005-2007 年(B 组)期间,使用调强放疗(IMRT)和可变时长雄激素剥夺治疗(ADT)连续识别接受根治性放疗的中高危局限性 PCa 患者。与 B 组患者没有每日 IGRT 不同,A 组患者接受每日在线成像引导(IGRT),使用锥形束计算机断层扫描(CBCT)。在报告人口统计学、临床病理特征和治疗细节后,我们比较了两组患者接受 RTOG/CTCAE 标准分级的急性(治疗后 3 个月内)和晚期 RT 诱导毒性。进行单变量/多变量分析(UVA/MVA),以确定与 RT 相关副作用的独立预测因素。
我们能够确定符合纳入标准的 257 例患者。总体而言,中位年龄为 73 岁(48-85 岁),67%为中危患者,47%接受 ADT。A 组 72 例患者接受容积调强弧形治疗(VMAT),B 组 185 例患者接受分步静态 IMRT。除 A 组患者的 3 级不良事件比例更高、中位总剂量更高(79.2 与 74 Gy)、骨盆淋巴结放疗更多(p <0.05)外,两组的临床病理特征和治疗细节无差异。尽管两组的急性毒性相似,但 B 组晚期毒性评分更高,晚期泌尿生殖系统不良反应更严重(P=0.008),晚期下消化道毒性无差异。多变量分析显示,缺乏每日 CBCT、非裔美国人种族和更高的合并症是晚期毒性的独立预测因素。
每日 CBCT 的 IMRT 可安全地进行剂量递增 IMRT,改善高危前列腺癌的毒性谱。