Departments of Clinical Pathology, National Liver Institute, Menoufia University, Egypt.
Hepatology, National Liver Institute-Menoufia University, Egypt.
Asian Pac J Cancer Prev. 2021 Jan 1;22(1):267-275. doi: 10.31557/APJCP.2021.22.1.267.
Portal vein thrombosis (PVT) might be a catastrophic event complicating liver cirrhosis and hepatocellular carcinoma (HCC).
role of JAK2 RS V617F mutation as a risk factor for PVT development in liver cirrhosis and HCC.
A case control study conducted on 100 PVT patients (76 HCC and 24 liver cirrhosis) additionally, 100 healthy individuals used as a control group. PVT was diagnosed incidentally by Doppler ultrasound during routine follow-up HCC screening. Prothrombin G20210A mutation, MTHFR mutation, Factor V Leiden mutation (VFL), antithrombin III (ATIII), protein C, S, and antiphospholipid antibodies, along with JAK2 RS V617F mutation by real-time polymerase chain reaction all were analyzed.
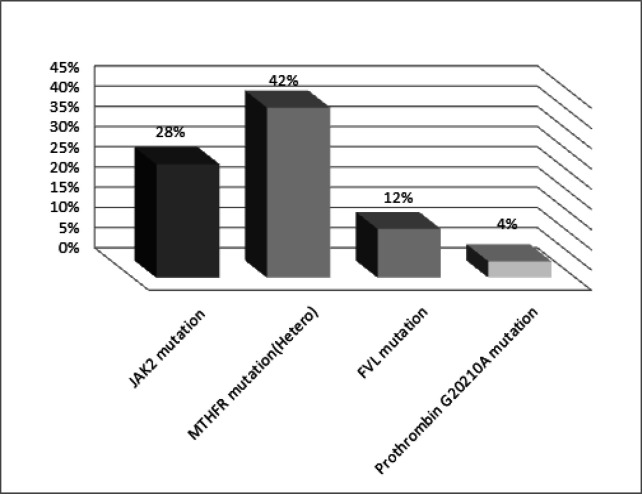
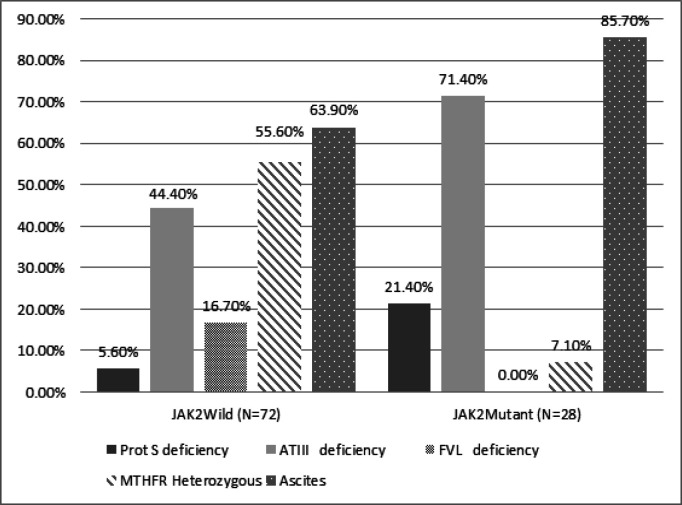
Patients with PVT were significantly older (p <0.001), thrombocytopenic (p <0.001), with high alkaline phosphatase (p <0.001). JAK2 RS V617F mutation was found in 28/100 (28%) in idiopathic PVT complicating liver cirrhosis and hepatocellular carcinoma. Cases with positive JAK2 rs V617F mutation were significantly accompanied by protein S deficiency (P 0.03), LA absence (p 0.06), and high frequency of ascites (P 0.03). While, the MTHFR heterozygous mutation (p0.001), ATIII (P 0.02), and VFL (P 0.01) were more frequent with negative JAK2 rs V617F mutation. The comparison between demographic data and thrombophilic parameters in PVT cases revealed that no significant differences were recorded except for male gender, Diabetes Mellitus, splenomegaly significantly increased among HCC cases (p <0.05).
JAK2 rs V617F mutation must be considered in any case of PVT with liver cirrhosis and hepatocellular carcinoma without identified thrombophilic risk factors, with potential considerations of evolving myeloproliferative disorders. New diagnostic and therapeutic implications are still awaited.
门静脉血栓形成(PVT)可能是肝硬化和肝细胞癌(HCC)的灾难性并发症。
JAK2 RS V617F 突变作为肝硬化和 HCC 中 PVT 发展的危险因素的作用。
对 100 例 PVT 患者(76 例 HCC 和 24 例肝硬化)进行病例对照研究,另外选择 100 例健康个体作为对照组。PVT 通过多普勒超声在常规 HCC 筛查期间偶然诊断。分析了凝血酶原 G20210A 突变、MTHFR 突变、因子 V Leiden 突变(VFL)、抗凝血酶 III(ATIII)、蛋白 C、S 和抗磷脂抗体以及实时聚合酶链反应的 JAK2 RS V617F 突变。
PVT 患者年龄明显较大(p<0.001),血小板减少(p<0.001),碱性磷酸酶升高(p<0.001)。在特发性 PVT 合并肝硬化和肝细胞癌中发现 JAK2 RS V617F 突变 28/100(28%)。阳性 JAK2 rs V617F 突变的病例明显伴有蛋白 S 缺乏症(P<0.03)、LA 缺失(p<0.06)和腹水发生率高(P<0.03)。而 MTHFR 杂合突变(p0.001)、ATIII(P<0.02)和 VFL(P<0.01)在阴性 JAK2 rs V617F 突变中更为常见。在 PVT 病例的人口统计学数据和血栓形成参数比较中,除了男性、糖尿病和脾肿大在 HCC 病例中明显增加(p<0.05)外,没有记录到显著差异。
在没有明确血栓形成危险因素的任何情况下,在肝硬化和肝细胞癌伴 PVT 的情况下,都必须考虑 JAK2 rs V617F 突变,这可能提示存在骨髓增生性疾病。新的诊断和治疗意义仍在等待。