Division of Cardiology, Department of Internal Medicine and Hubei Key Laboratory of Genetics and Molecular Mechanism of Cardiologic Disorders, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430030, China.
The Center for Cardiovascular Genetics, The Brown Foundation Institute of Molecular Medicine, The University of Texas Health Science Center, Houston, TX, 77030, USA.
Acta Pharmacol Sin. 2021 Oct;42(10):1567-1574. doi: 10.1038/s41401-020-00595-z. Epub 2021 Jan 28.
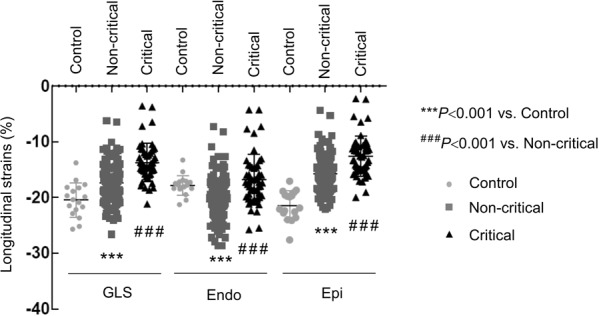
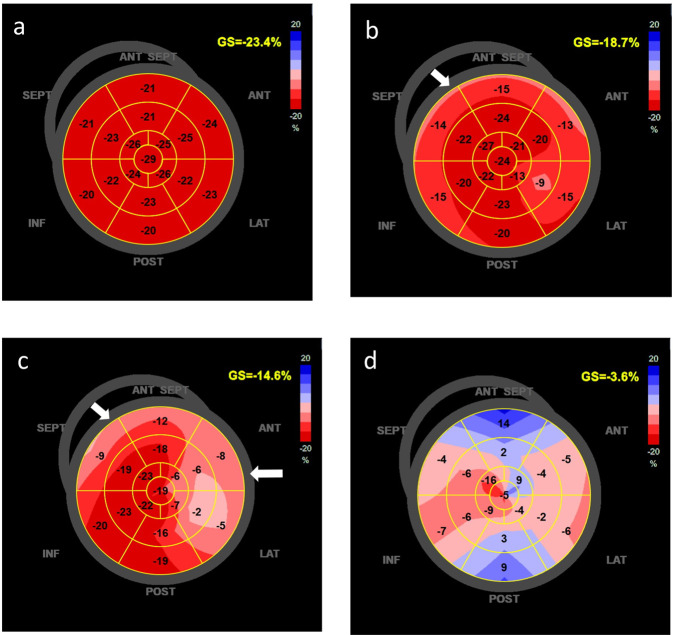
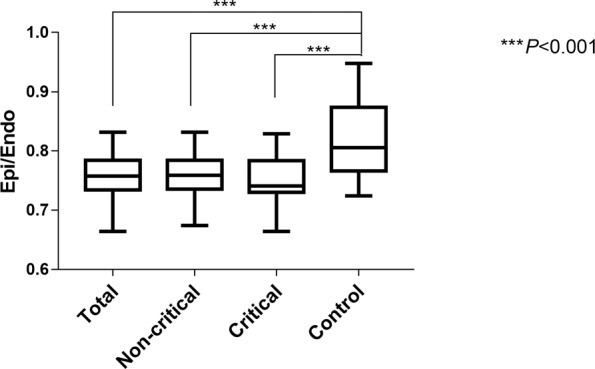
COVID-19 is a multiorgan systemic inflammatory disease caused by SARS-CoV-2 virus. Patients with COVID-19 often exhibit cardiac dysfunction and myocardial injury, but imaging evidence is lacking. In the study we detected and evaluated the severity of myocardial dysfunction in COVID-19 patient population using two-dimensional speckle-tracking echocardiography (2-D STE). A total of 218 consecutive patients with confirmed diagnosis of COVID-19 who had no underlying cardiovascular diseases were enrolled and underwent transthoracic echocardiography. This study cohort included 52 (23.8%) critically ill and 166 noncritically ill patients. Global longitudinal strains (GLSs) and layer-specific longitudinal strains (LSLSs) were obtained using 2-D STE. Changes in GLS were correlated with the clinical parameters. We showed that GLS was reduced (<-21.0%) in about 83% of the patients. GLS reduction was more common in critically sick patients (98% vs. 78.3%, P < 0.001), and the mean GLS was significantly lower in the critically sick patients than those noncritical (-13.7% ± 3.4% vs. -17.4% ± 3.2%, P < 0.001). The alteration of GLS was more prominent in the subepicardium than in the subendocardium (P < 0.001). GLS was correlated to mean serum pulse oxygen saturation (SpO, RR = 0.42, P < 0.0001), high-sensitive C-reactive protein (hsCRP, R = -0.20, P = 0.006) and inflammatory cytokines, particularly IL-6 (R = -0.21, P = 0.003). In conclusions, our results demonstrate that myocardial dysfunction is common in COVID-19 patients, particularly those who are critically sick. Changes in indices of myocardial strain were associated with indices of inflammatory markers and hypoxia, suggesting partly secondary nature of myocardial dysfunction.
COVID-19 是由 SARS-CoV-2 病毒引起的多器官系统性炎症疾病。COVID-19 患者常表现出心脏功能障碍和心肌损伤,但影像学证据不足。在本研究中,我们使用二维斑点追踪超声心动图(2-D STE)检测并评估了 COVID-19 患者人群中心肌功能障碍的严重程度。共纳入 218 例经确诊的 COVID-19 患者,且均无基础心血管疾病,行经胸超声心动图检查。本研究队列包括 52 例(23.8%)危重症患者和 166 例非危重症患者。使用 2-D STE 获得整体纵向应变(GLS)和节段性纵向应变(LSLS)。GLS 的变化与临床参数相关。结果显示,约 83%的患者 GLS 降低(<-21.0%)。危重症患者 GLS 降低更为常见(98% vs. 78.3%,P < 0.001),且危重症患者的平均 GLS 明显低于非危重症患者(-13.7%±3.4% vs. -17.4%±3.2%,P < 0.001)。GLS 的改变在心外膜下比心内膜下更为显著(P < 0.001)。GLS 与平均血清脉搏血氧饱和度(SpO,RR = 0.42,P < 0.0001)、高敏 C 反应蛋白(hsCRP,R = -0.20,P = 0.006)和炎症细胞因子(特别是 IL-6,R = -0.21,P = 0.003)呈正相关。总之,我们的结果表明 COVID-19 患者,特别是危重症患者,心肌功能障碍很常见。心肌应变指标的变化与炎症标志物和缺氧指标相关,提示心肌功能障碍部分具有继发性特征。