The Study Center of the German Surgical Society (SDGC), University of Heidelberg, Im Neuenheimer Feld 110, 69120, Heidelberg, Germany.
Department of General, Visceral and Transplantation Surgery, University of Heidelberg, Im Neuenheimer Feld 110, 69120, Heidelberg, Germany.
J Gastrointest Surg. 2021 Oct;25(10):2600-2609. doi: 10.1007/s11605-020-04904-z. Epub 2021 Jan 28.
Patients undergoing relaparotomy are generally underrepresented in trials, despite how common the procedure is in clinical practice. The aim of this trial was to determine standard of care and gain evidence of intra- and postoperative outcomes for patients undergoing relaparotomy compared to primary laparotomy.
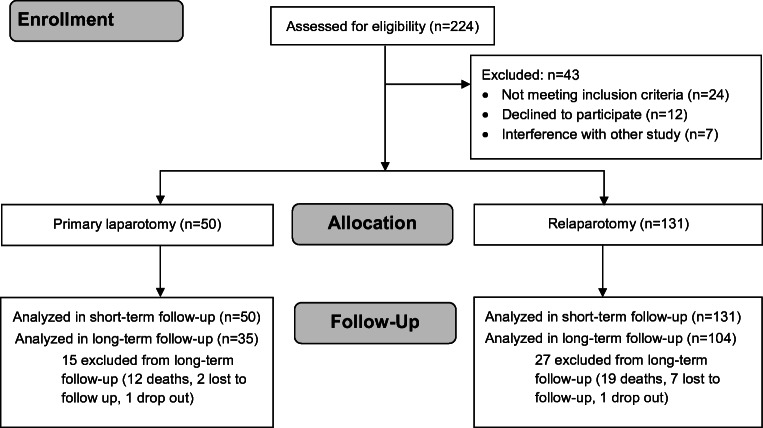
In this single-center controlled clinical trial, adult patients scheduled for elective abdominal surgery via relaparotomy or primary laparotomy were consecutively screened for eligibility. The perioperative course was monitored prospectively in five study visits during hospital stay and one study visit 1 year after surgery. Intraoperative standards, short and long-term outcomes were statistically explored at a level of significance of 5%.
A total of 131 patients with relaparotomy and 50 patients with primary laparotomy were analyzed. In the relaparotomy group, the access to the abdomen took longer (23.5 min vs. 8.8 min; p = < 0.001) and the peritoneal adhesion index was higher (10.8 vs. 0.4; p = < 0.001). Inadvertent enterotomies were more frequent in the relaparotomy group (relaparotomy 0.3 versus primary laparotomy: 0.0; p = 0.002). The overall comprehensive complication index and rates of surgical site infection and wound dehiscence with evisceration were not different between the two groups. At long-term follow-up, rates of incisional hernia did not differ (relaparotomy: n = 12/104 (11.5%); primary laparotomy: n = 7/35 (20.0%); p = 0.208).
In this first prospective comparison of relaparotomy with primary laparotomy, inadvertent enterotomies were more frequent in the relaparotomy group. However, contrary to previous retrospective studies, the risk of complications and incisional hernias was not increased compared to primary laparotomy.
Deutsches Register Klinischer Studien ( www.germanctr.de ): DRKS00013001.
尽管剖腹探查术在临床实践中很常见,但接受再次剖腹探查术的患者通常在临床试验中代表性不足。本试验旨在确定标准治疗方法,并为接受再次剖腹探查术与初次剖腹探查术的患者提供围手术期和术后结果的证据。
在这项单中心对照临床试验中,连续筛选择期接受再次剖腹探查术或初次剖腹探查术的成年患者是否符合入选标准。在住院期间进行了五次研究访视,以及术后 1 年进行了一次研究访视,以前瞻性监测围手术期过程。在 5%的显著性水平上,对术中标准、短期和长期结果进行了统计学探讨。
共分析了 131 例再次剖腹探查术患者和 50 例初次剖腹探查术患者。在再次剖腹探查组中,进入腹部的时间更长(23.5 分钟 vs. 8.8 分钟;p < 0.001),腹膜粘连指数更高(10.8 分 vs. 0.4 分;p < 0.001)。在再次剖腹探查组中更频繁地发生意外肠切开(再次剖腹探查术 0.3% vs. 初次剖腹探查术 0.0%;p = 0.002)。两组的综合并发症指数以及手术部位感染和伤口裂开伴内脏脱出的发生率无差异。在长期随访中,切口疝的发生率也无差异(再次剖腹探查术:n = 12/104(11.5%);初次剖腹探查术:n = 7/35(20.0%);p = 0.208)。
在这项再次剖腹探查术与初次剖腹探查术的首次前瞻性比较中,再次剖腹探查组更频繁地发生意外肠切开。然而,与之前的回顾性研究相反,与初次剖腹探查术相比,并发症和切口疝的风险并未增加。
德国临床试验注册中心(www.germanctr.de):DRKS00013001。