Department of General, Visceral and Transplantation Surgery, University of Heidelberg, Im Neuenheimer Feld 110, 69120, Heidelberg, Germany.
The Study Center of the German Surgical Society (SDGC), University of Heidelberg, Im Neuenheimer Feld 110, 69120, Heidelberg, Germany.
Langenbecks Arch Surg. 2020 Jun;405(4):427-434. doi: 10.1007/s00423-020-01903-1. Epub 2020 Jun 6.
Patients undergoing relaparotomy are generally underrepresented in clinical trials, despite how common the procedure is in clinical practice. Specifically, techniques for re-do abdominal wall closure have never been evaluated in a randomised-controlled trial. The aim of this trial was to identify the optimal abdominal wall closure technique in patients undergoing relaparotomy.
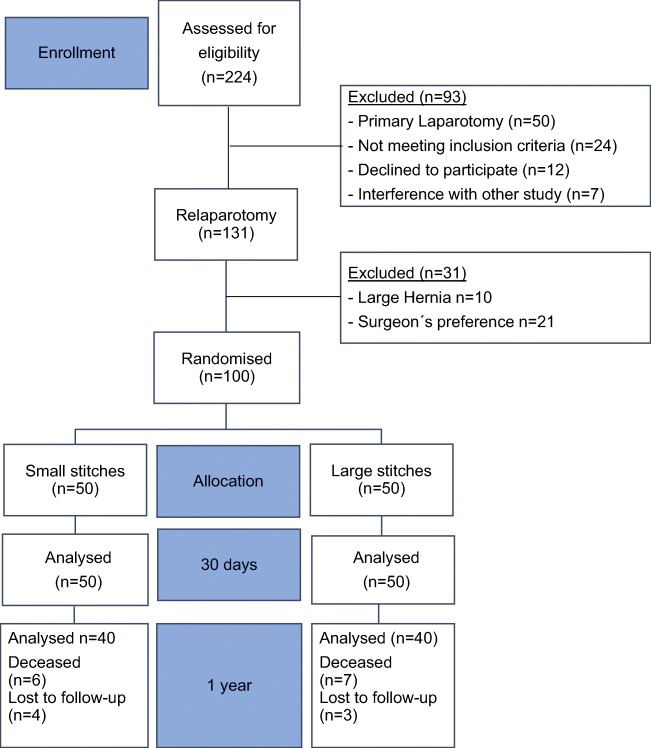
In this monocentric, randomised feasibility trial, patients scheduled for elective relaparotomy were randomised to abdominal wall closure with either the small stitches technique, using Monomax® 2-0, or the large stitches technique, using PDS II® 1 loop. Patients' postoperative courses were followed for 1 year after the index operation. Effectiveness and safety outcomes were compared at a level of significance of 5% between the two techniques.
A total of 100 out of 131 patients (76.3%) were evenly randomised to the small stitches and large stitches groups. The time for abdominal wall closure did not differ between the two techniques (small stitches 27.5 ± 9.5 min versus large stitches 25.3 ± 12.4 min; p = 0.334). The overall comprehensive complication index was 14.4 ± 15.5 in the small stitches group and 19.9 ± 23.4 in the large stitches group (p = 0.168). Specifically, rates of surgical site infection (small stitches 30.0% versus large stitches 36.0%; p = 0.524) and burst abdomen (small stitches 4.0% versus large stitches 0.0%; p = 0.495) did not differ. After 1 year, incisional hernia rate was 7.5% in the small stitches group and 10.0% in the large stitches group (p > 0.999).
Both abdominal wall closure techniques investigated in this trial were feasible in relaparotomy patients. This exploratory trial revealed no noticeable difference in the effectiveness or safety of the small stitches technique with Monomax® 2-0 versus the large stitches technique with PDS II® 1 loop. Therefore, surgeons should stay with their preferred suture technique in relaparotomy patients.
Deutsches Register Klinischer Studien ( www.germanctr.de ): DRKS00013001.
尽管剖腹术在临床实践中很常见,但接受再次剖腹术的患者在临床试验中通常代表性不足。具体来说,用于重新关闭腹壁的技术从未在随机对照试验中进行过评估。本试验的目的是确定再次剖腹术患者中最佳的腹壁关闭技术。
在这项单中心、随机可行性试验中,计划接受择期再次剖腹术的患者被随机分为两组,分别采用 Monomax® 2-0 缝线的小缝线技术或 PDS II® 1 缝线的大缝线技术进行腹壁关闭。对患者的术后病程进行了 1 年的随访。在 5%的显著性水平上比较了两种技术的有效性和安全性结局。
共有 131 名患者中的 100 名(76.3%)被平均随机分为小缝线组和大缝线组。两种技术的腹壁关闭时间无差异(小缝线组 27.5 ± 9.5 分钟,大缝线组 25.3 ± 12.4 分钟;p = 0.334)。小缝线组的综合并发症指数为 14.4 ± 15.5,大缝线组为 19.9 ± 23.4(p = 0.168)。具体而言,手术部位感染率(小缝线组 30.0%,大缝线组 36.0%;p = 0.524)和腹部破裂率(小缝线组 4.0%,大缝线组 0.0%;p = 0.495)没有差异。1 年后,小缝线组的切口疝发生率为 7.5%,大缝线组为 10.0%(p > 0.999)。
本试验中研究的两种腹壁关闭技术在再次剖腹术患者中均可行。这项探索性试验表明,采用 Monomax® 2-0 的小缝线技术与采用 PDS II® 1 缝线的大缝线技术在有效性和安全性方面没有明显差异。因此,外科医生应在再次剖腹术患者中坚持使用他们首选的缝合技术。
德国临床试验注册中心(www.germanctr.de):DRKS00013001。