Division of Immunobiology, Department of Pediatrics, Cincinnati Children's Hospital Medical Center, University of Cincinnati, Cincinnati, OH.
Division of Bone Marrow Transplantation and Immune Deficiency, Cancer and Blood Diseases Institute, Cincinnati Children's Hospital Medical Center, Cincinnati, OH.
Blood. 2021 Apr 29;137(17):2337-2346. doi: 10.1182/blood.2020009499.
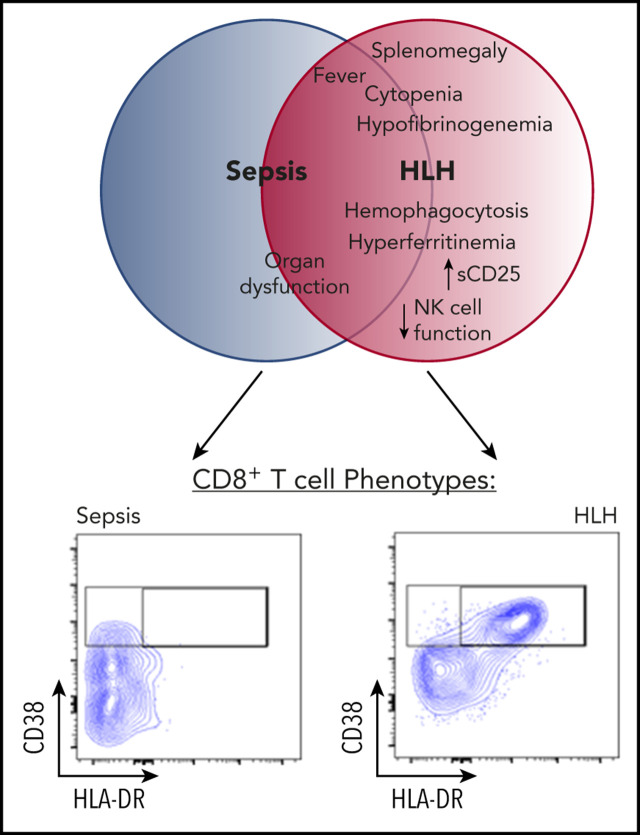
Hemophagocytic lymphohistiocytosis (HLH) is a fatal disorder of immune hyperactivation that has been described as a cytokine storm. Sepsis due to known or suspected infection has also been viewed as a cytokine storm. Although clinical similarities between these syndromes suggest similar immunopathology and may create diagnostic uncertainty, distinguishing them is critical as treatments are widely divergent. We examined T-cell profiles from children with either HLH or sepsis and found that HLH is characterized by acute T-cell activation, in clear contrast to sepsis. Activated T cells in patients with HLH were characterized as CD38high/HLA-DR+ effector cells, with activation of CD8+ T cells being most pronounced. Activated T cells were type 1 polarized, proliferative, and displayed evidence of recent and persistent activation. Circulating activated T cells appeared to be broadly characteristic of HLH, as they were seen in children with and without genetic lesions or identifiable infections and resolved with conventional treatment of HLH. Furthermore, we observed even greater activation and type 1 polarization in tissue-infiltrating T cells, described here for the first time in a series of patients with HLH. Finally, we observed that a threshold of >7% CD38high/HLA-DR+ cells among CD8+ T cells had strong positive and negative predictive value for distinguishing HLH from early sepsis or healthy controls. We conclude that the cytokine storm of HLH is marked by distinctive T-cell activation whereas early sepsis is not, and that these 2 syndromes can be readily distinguished by T-cell phenotypes.
噬血细胞性淋巴组织细胞增生症(HLH)是一种免疫过度激活的致命疾病,可被视为细胞因子风暴。由于已知或疑似感染引起的败血症也被视为细胞因子风暴。尽管这些综合征之间存在临床相似性,提示存在相似的免疫病理学,并可能导致诊断不确定,但区分它们至关重要,因为治疗方法有很大差异。我们检查了患有 HLH 或败血症的儿童的 T 细胞谱,发现 HLH 的特征是急性 T 细胞激活,与败血症形成鲜明对比。HLH 患者的活化 T 细胞表现为 CD38high/HLA-DR+效应细胞,其中 CD8+T 细胞的激活最为明显。活化的 T 细胞呈 1 型极化,增殖,并显示出最近和持续激活的证据。循环活化 T 细胞似乎广泛存在于 HLH 中,因为它们存在于有遗传病变或可识别感染的儿童和没有遗传病变或可识别感染的儿童中,并且随着 HLH 的常规治疗而得到解决。此外,我们观察到组织浸润性 T 细胞中甚至更大的激活和 1 型极化,这在一组 HLH 患者中首次描述。最后,我们观察到 CD8+T 细胞中 CD38high/HLA-DR+细胞比例>7%对区分 HLH 与早期败血症或健康对照具有很强的阳性和阴性预测值。我们得出的结论是,HLH 的细胞因子风暴以独特的 T 细胞激活为特征,而早期败血症则不然,并且这两种综合征可以通过 T 细胞表型轻易区分。