Picard Véronique, Guitton Corinne, Mansour-Hendili Lamisse, Jondeau Bernard, Bendélac Laurence, Denguir Maha, Demagny Julien, Proulle Valérie, Galactéros Frédéric, Garçon Loic
Service d'Hématologie Biologique, Assistance Publique-Hôpitaux de Paris, Hôpital Bicêtre, Hôpitaux Universitaires Paris-Saclay, Le Kremlin-Bicêtre, France.
Faculté de Pharmacie, Université Paris-Saclay, Châtenay-Malabry, France.
Front Physiol. 2021 Jan 14;11:602109. doi: 10.3389/fphys.2020.602109. eCollection 2020.
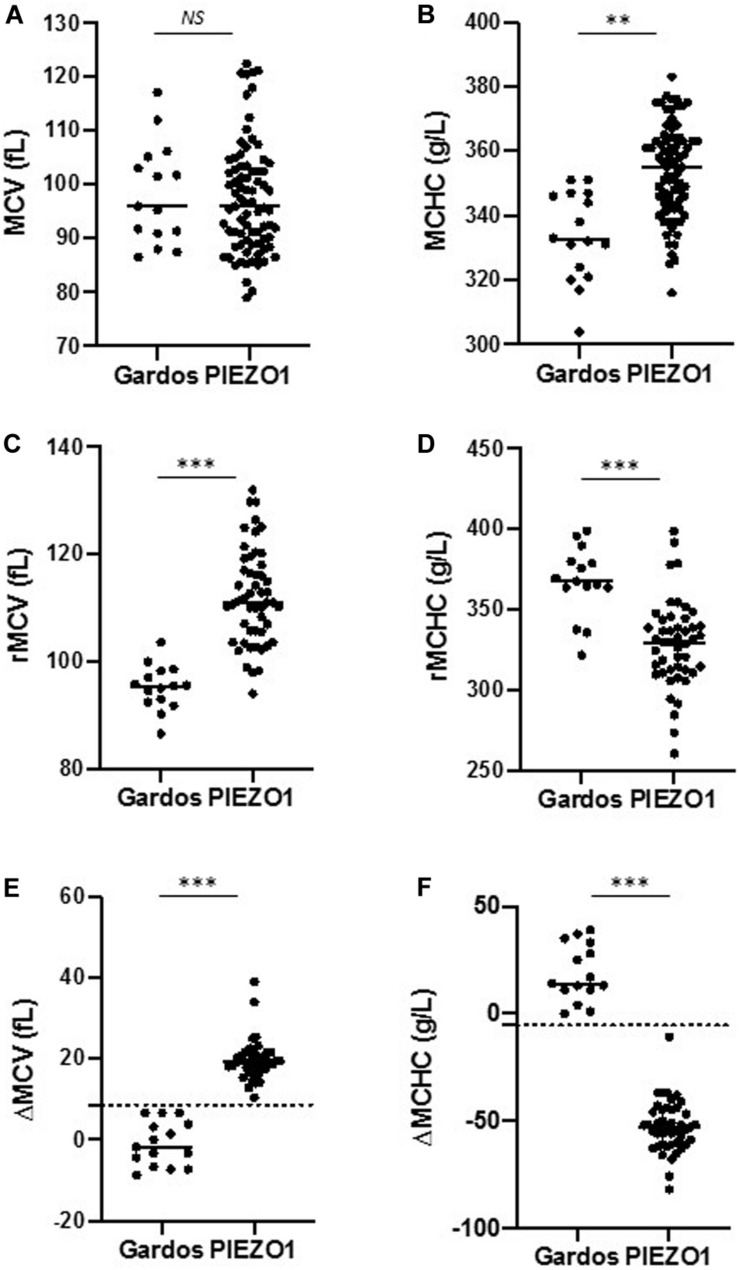
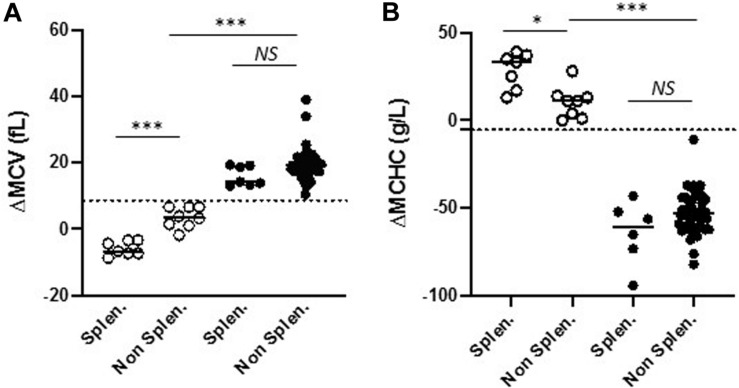
Gardos channelopathy (Gardos-HX) or type 2 stomatocytosis/xerocytosis is a hereditary hemolytic anemia due to mutations in the gene. It is rarer than inherited type 1 xerocytosis due to mutations (Piezo1-HX) and its diagnosis is difficult given the absence of a specific clinical or biological phenotype. We report here that this diagnosis can be sped up using red blood cell (RBC) indices performed on an ADVIA 2120 (Siemens) analyzer, which measures reticulocyte mean corpuscular volume (rMCV) and mean corpuscular hemoglobin concentration (rMCHC). We studied reticulocyte indices in 3 new and 12 described patients (8 families) with Gardos-HX, 11 subjects presented the recurrent p.Arg352His mutation, 4 cases (two families) carried a private mutation. They were compared to 79 described patients (49 families) with Piezo1-HX. Surprisingly, in Gardos-HX cases, rMCV revealed to be smaller than MCV and rMCHC higher than MCHC, in contrast with normal or Piezo1-HX RBC. Consequently, ΔMCV (rMCV-MCV) was -0.9 ± 5 fL vs. 19.8 ± 3 fL ( < 0.001) in Gardos compared with Piezo1-HX and ΔMCHC (rMCHC-MCHC) was 18.7 ± 13 vs. -50 ± 8.7 g/L ( < 0.001). A threshold of 8.6 fL for ΔMCV and -5.5 g/L for ΔMCHC could discriminate between Gardos and Piezo1-HX with 100% sensitivity and specificity, regardless of age, mutation or splenectomy status. Consequently, we showed that reticulocytes indices are useful to suggest Gardos-HX on blood count results, allowing to rapidly target these patients for gene analysis. In addition, these parameters may prove useful as a 'functional tool' in interpreting new variants.
加尔多斯通道病(加尔多斯 - HX)或2型口形细胞增多症/干皮症是一种由于该基因发生突变导致的遗传性溶血性贫血。它比因Piezo1基因突变(Piezo1 - HX)导致的遗传性1型干皮症更为罕见,并且由于缺乏特定的临床或生物学表型,其诊断较为困难。我们在此报告,使用ADVIA 2120(西门子)分析仪检测红细胞(RBC)指标可以加快这一诊断过程,该分析仪可测量网织红细胞平均红细胞体积(rMCV)和平均红细胞血红蛋白浓度(rMCHC)。我们研究了3例新诊断的和12例已报道的加尔多斯 - HX患者(8个家系)的网织红细胞指标,其中11例患者存在复发性p.Arg352His突变,4例(两个家系)携带一个私人突变。将他们与79例已报道的Piezo1 - HX患者(49个家系)进行比较。令人惊讶的是,在加尔多斯 - HX病例中,与正常或Piezo1 - HX红细胞相反,rMCV显示小于MCV,rMCHC高于MCHC。因此与Piezo1 - HX相比,加尔多斯病例的ΔMCV(rMCV - MCV)为 - 0.9±5 fL,而Piezo1 - HX为19.8±3 fL(P < 0.001),ΔMCHC(rMCHC - MCHC)为18.7±13 vs. - 50±8.7 g/L(P < 0.001)。ΔMCV的阈值为8.6 fL和ΔMCHC的阈值为 - 5.5 g/L可以区分加尔多斯病和Piezo1 - HX,敏感性和特异性均为100%,无论年龄、突变或脾切除状态如何。因此,我们表明网织红细胞指标有助于根据血常规结果提示加尔多斯 - HX,从而能够迅速将这些患者作为基因分析的目标。此外,这些参数可能被证明是解释新变异的“功能工具”。