Hashemi Djawid, Motzkus Laura, Blum Moritz, Kraft Robin, Tanacli Radu, Tahirovic Elvis, Doeblin Patrick, Zieschang Victoria, Zamani S Mahsa, Kelm Marcus, Kuehne Titus, Pieske Burkert, Alogna Alessio, Edelmann Frank, Duengen Hans-Dirk, Kelle Sebastian
Department of Internal Medicine and Cardiology, Charité-Universitätsmedizin Berlin, Campus Virchow Klinikum, Berlin, Germany.
DZHK (German Centre for Cardiovascular Research), partner site Berlin, Berlin, Germany.
ESC Heart Fail. 2021 Apr;8(2):890-897. doi: 10.1002/ehf2.13193. Epub 2021 Feb 4.
Although heart failure (HF) is a leading cause for hospitalization and mortality, normalized and comparable non-invasive assessment of haemodynamics and myocardial action remains limited. Moreover, myocardial deformation has not been compared between the guideline-defined HF entities. The distribution of affected and impaired segments within the contracting left ventricular (LV) myocardium have also not been compared. Therefore, we assessed myocardial function impairment by strain in patients with HF and control subjects by magnetic resonance imaging after clinically phenotyping these patients.
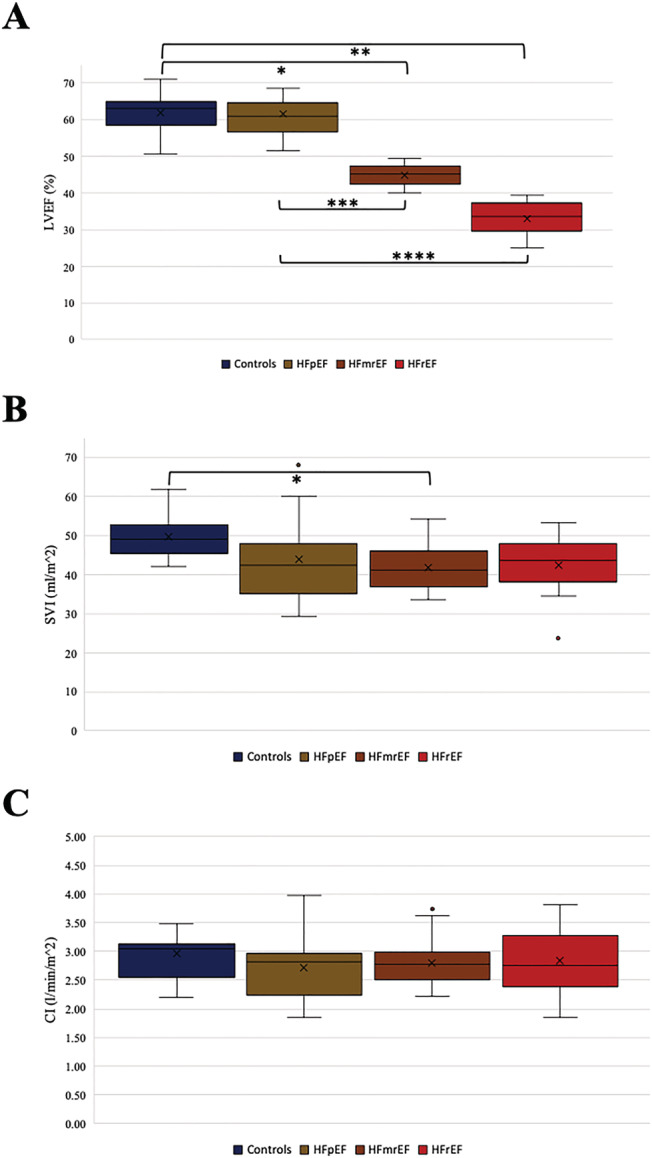
This prospective study conducted at two centres in Germany between 2017 and 2018 enrolled stable outpatient subjects with HF [n = 56, including HF with reduced ejection fraction (HFrEF), HF with mid-range ejection fraction (HFmrEF), and HF with preserved ejection fraction (HFpEF)] and a control cohort (n = 12). Parameters assessed included measures for external myocardial function, for example, cardiac index and myocardial deformation measurements by cardiovascular magnetic resonance imaging, left ventricular global longitudinal strain (GLS), the global circumferential strain (GCS) and the regional distribution of segment deformation within the LV myocardium, as well as basic phenotypical characteristics. Comparison of the cardiac indices at rest showed no differences neither between the HF groups nor between the control group and HF patients (one-way ANOVA P = 0.70). The analysis of the strain data revealed differences between all groups in both LV GLS (One-way ANOVA: P < 0.01. Controls vs. HFpEF: -20.48 ± 1.62 vs. -19.27 ± 1.25. HFpEF vs. HFmrEF: -19.27 ± 1.25 vs. -15.72 ± 2.76. HFmrEF vs. HFrEF: -15.72 ± 2.76 vs. -11.51 ± 3.97.) and LV GCS (One-way ANOVA: P < 0.01. Controls vs. HFpEF: -19.74 ± 2.18 vs. -17.47 ± 2.10. HFpEF vs. HFmrEF: -17.47 ± 2.10 vs. -12.78 ± 3.47. HFrEF: -11.41 ± 3.27). Comparing the segment deformation distribution patterns highlighted the discriminating effect between the groups was much more prominent between the groups (one-way ANOVA P < 0.01) when compared by a score combining regional effects and a global view on the LV. Further analyses of the patterns among the segments affected showed that while the LVEF is preserved in HFpEF, the segments impaired in their contractility are located in the ventricular septum. The worse the LVEF is, the more segments are affected, but the septum remains an outstanding location with the most severe contractility impairment throughout the HF entities.
While cardiac index at rest did not differ significantly between controls and stable HF patients suffering from HFrEF, HFmrEF, or HFpEF, the groups did differ significantly in LV GLS and LV GCS values. Regional strain analysis revealed that the LV septum is the location affected most, with reduced values already visible in HFpEF and further reductions in HFmrEF and HFrEF.
尽管心力衰竭(HF)是住院和死亡的主要原因,但血流动力学和心肌活动的标准化及可比较的非侵入性评估仍然有限。此外,尚未对指南定义的HF实体之间的心肌变形进行比较。收缩期左心室(LV)心肌内受影响和受损节段的分布也未进行比较。因此,我们在对这些患者进行临床表型分析后,通过磁共振成像评估了HF患者和对照受试者的心肌应变功能损害。
这项前瞻性研究于2017年至2018年在德国的两个中心进行,纳入了稳定的门诊HF患者[n = 56,包括射血分数降低的HF(HFrEF)、射血分数中等范围的HF(HFmrEF)和射血分数保留的HF(HFpEF)]以及一个对照队列(n = 12)。评估的参数包括外部心肌功能的测量指标,例如通过心血管磁共振成像测量心脏指数和心肌变形、左心室整体纵向应变(GLS)、整体圆周应变(GCS)以及LV心肌内节段变形的区域分布,以及基本的表型特征。静息时心脏指数的比较显示,HF组之间以及对照组与HF患者之间均无差异(单因素方差分析P = 0.70)。应变数据分析显示,所有组在LV GLS(单因素方差分析:P < 0.01。对照组与HFpEF:-20.48 ± 1.62 vs. -19.27 ± 1.25。HFpEF与HFmrEF:-19.27 ± 1.25 vs. -15.72 ± 2.76。HFmrEF与HFrEF:-15.72 ± 2.76 vs. -11.51 ± 3.97。)和LV GCS(单因素方差分析:P < 0.01。对照组与HFpEF:-19.74 ± 2.18 vs. -17.47 ± 2.10。HFpEF与HFmrEF:-17.47 ± 2.10 vs. -12.78 ± 3.47。HFrEF:-11.41 ± 3.27)方面均存在差异。比较节段变形分布模式发现,与通过结合区域效应和LV整体视图的评分进行比较时相比,组间的区分效应在组间更为显著(单因素方差分析P < 0.01)。对受影响节段的模式进行进一步分析表明,虽然HFpEF中LVEF得以保留,但收缩力受损的节段位于室间隔。LVEF越差,受影响的节段越多,但在整个HF实体中,室间隔仍然是收缩力受损最严重的突出部位。
虽然静息时心脏指数在对照组与患有HFrEF、HFmrEF或HFpEF的稳定HF患者之间无显著差异,但这些组在LV GLS和LV GCS值上存在显著差异。区域应变分析显示,LV室间隔是受影响最严重的部位,在HFpEF中已可见值降低,在HFmrEF和HFrEF中进一步降低。