Stroke Director, Southwest Healthcare System, 36485 Inland Valley Drive, Wildomar, CA 92595, United States; Neurosurgeon, Temecula Valley Neurosurgery, 25150 Hancock St. Suite 210, Murrieta CA 92562, United States.
UCSD Research Assistant, 9500 Gilman Dr., La Jolla, CA 92093, United States.
J Stroke Cerebrovasc Dis. 2021 Apr;30(4):105639. doi: 10.1016/j.jstrokecerebrovasdis.2021.105639. Epub 2021 Jan 26.
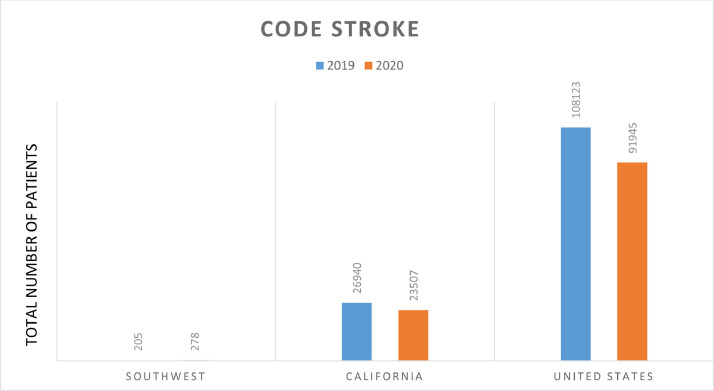
To examine the impact of the COVID-19 pandemic on stroke, the number of stroke patients, time since last known well (LKW), morbidity, and mortality of stroke patients in Southwest Healthcare System (SHS), California (CA) and the United States (US) were analyzed during 2019 and compared to 2020. Our hypothesis is that there are regional differences in stroke outcome depending on location during the COVID-19 study period which influences stroke epidemiology and clinical stroke practice.
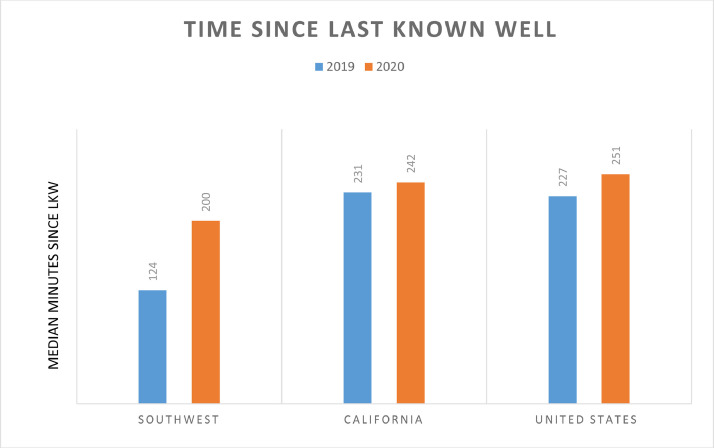
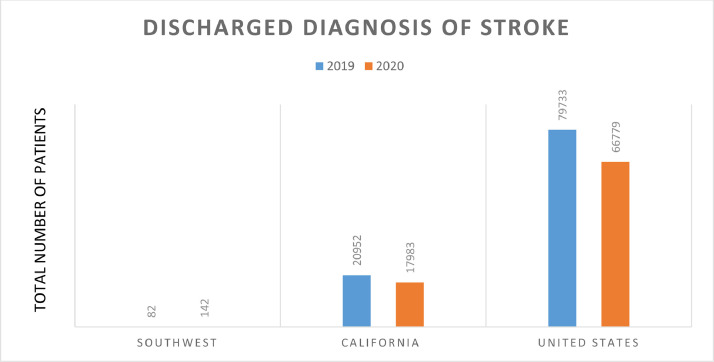
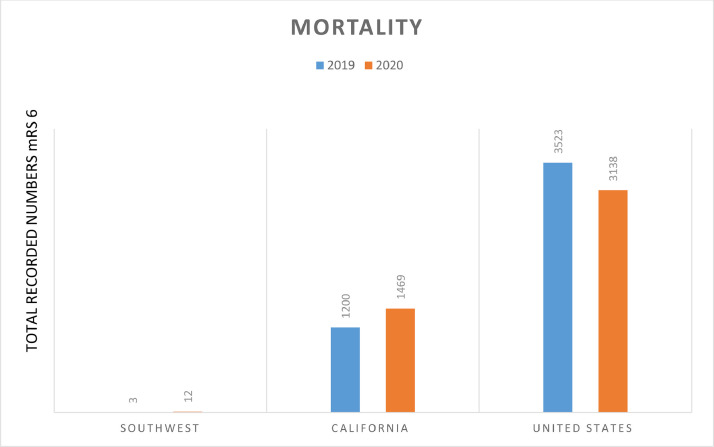
The American Heart Association's 'Get with the Guidelines' (GWTG) database was used to evaluate the following categories: code stroke, diagnosis of stroke upon discharge, inpatient mortality, modified Rankin Score (mRS) upon discharge (morbidity), and time since last known well (LKW). Stroke registry data from February through June 2019 and 2020 were collected for retrospective review.
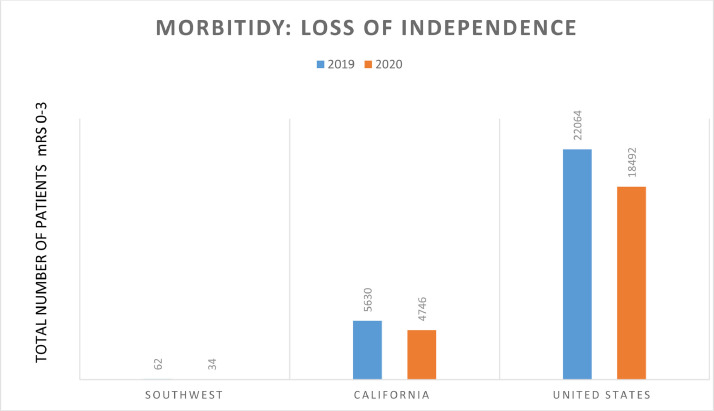
The total number of strokes decreased in the US and CA, but increased in SHS during the COVID-19 study period. The US and SHS demonstrated no change in stroke mortality, but CA demonstrated a higher stroke mortality during the COVID-19 pandemic. There was greater loss of independence with increased stroke morbidity in the US during the COVID-19 pandemic. There was a significant increase in time since LKW in the US and SHS, and an increase trend in time since LKW in CA during the COVID-19 study period.
To understand the impact of the COVID-19 pandemic on stroke epidemiology, we propose that all stroke inpatients should receive a SARS-CoV-2 detection test and this result be entered into the GWTG database. We demonstrate that the regional distribution of stroke mortality in the US changed during the COVID-19 study period, with increased stroke mortality in CA. Stroke morbidity throughout the US was significantly worse during the COVID-19 pandemic. We propose methods to address the impact of the COVID-19 pandemic on clinical stroke practice such as the use of mobile stroke units, clinical trials using anti-inflammation drugs on SARS-CoV-2 positive stroke patients, and COVID stroke rehabilitation centers.
为了研究 COVID-19 大流行对中风的影响,分析了加利福尼亚州(CA)和美国(US)西南医疗保健系统(SHS)中风患者的中风患者人数、距上次已知健康时间(LKW)、发病率和死亡率,并将 2019 年的结果与 2020 年的结果进行了比较。我们的假设是,在 COVID-19 研究期间,由于地理位置不同,中风结果存在区域差异,这会影响中风流行病学和临床中风实践。
使用美国心脏协会的“遵循指南”(GWTG)数据库评估以下类别:中风代码、出院时的中风诊断、住院死亡率、出院时的改良 Rankin 评分(mRS)(发病率)和距上次已知健康时间(LKW)。收集了 2019 年 2 月至 6 月和 2020 年的中风登记数据进行回顾性审查。
在 COVID-19 研究期间,美国和 CA 的中风总数减少,但 SHS 增加。美国和 SHS 显示中风死亡率没有变化,但 CA 在 COVID-19 大流行期间显示出更高的中风死亡率。在 COVID-19 大流行期间,美国的中风发病率更高,独立性丧失更大。在美国和 SHS 中,LKW 后的时间显著增加,在 CA 中,LKW 后的时间呈增加趋势。
为了了解 COVID-19 大流行对中风流行病学的影响,我们建议所有中风住院患者都应接受 SARS-CoV-2 检测,并且该结果应输入 GWTG 数据库。我们表明,在美国,COVID-19 研究期间,中风死亡率的区域分布发生了变化,CA 的中风死亡率增加。在 COVID-19 大流行期间,美国各地的中风发病率明显恶化。我们提出了一些方法来应对 COVID-19 大流行对临床中风实践的影响,例如使用移动中风单元、对 SARS-CoV-2 阳性中风患者进行抗炎药物临床试验以及 COVID 中风康复中心。