Taniguchi Ryosuke, Ono Shun, Isaji Toshihiko, Gorecka Jolanta, Lee Shin-Rong, Matsubara Yutaka, Yatsula Bogdan, Koizumi Jun, Nishibe Toshiya, Hoshina Katsuyuki, Dardik Alan
Vascular Biology and Therapeutics Program, Yale School of Medicine, New Haven.
Division of Vascular Surgery, The University of Tokyo, Bunkyo-ku, Tokyo.
JVS Vasc Sci. 2020;1:109-122. doi: 10.1016/j.jvssci.2020.07.003. Epub 2020 Jul 28.
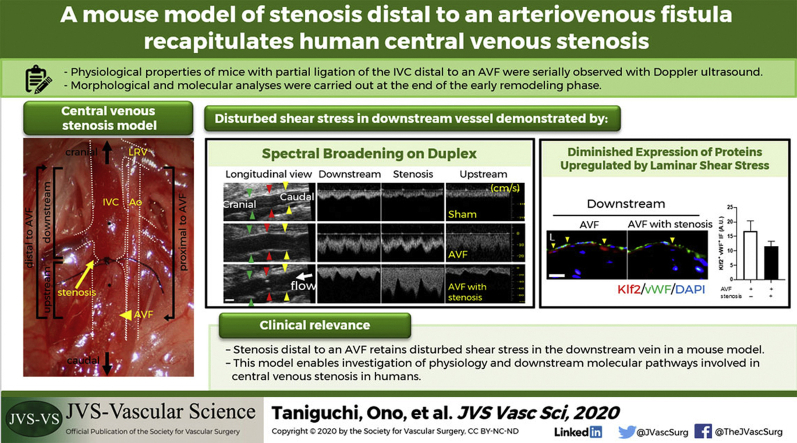
Central venous stenosis (CVS) is a major cause of arteriovenous fistula (AVF) failure. However, central veins are relatively inaccessible to study with conventional Doppler ultrasound methods. To understand mechanisms underlying AVF failure owing to CVS, an animal model was established that creates a stenosis distal to an AVF. We hypothesized that this mouse model will show comparable morphology and physiology to human CVS.
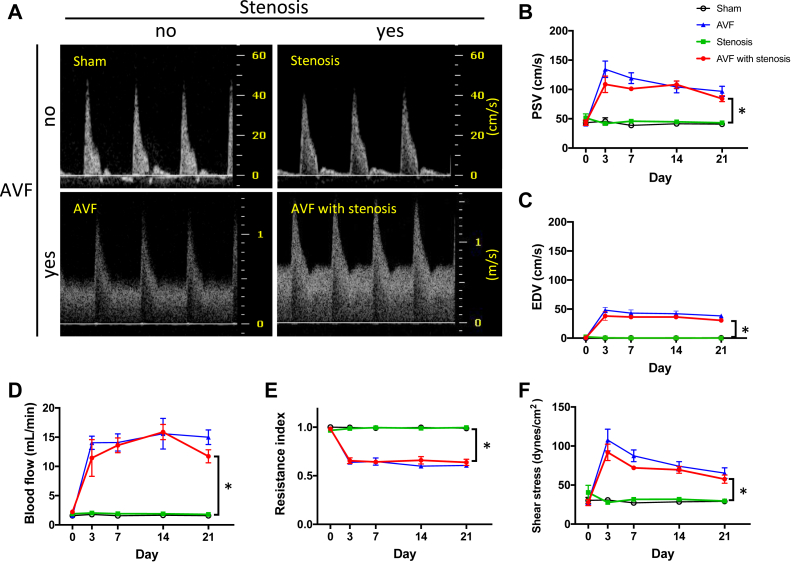
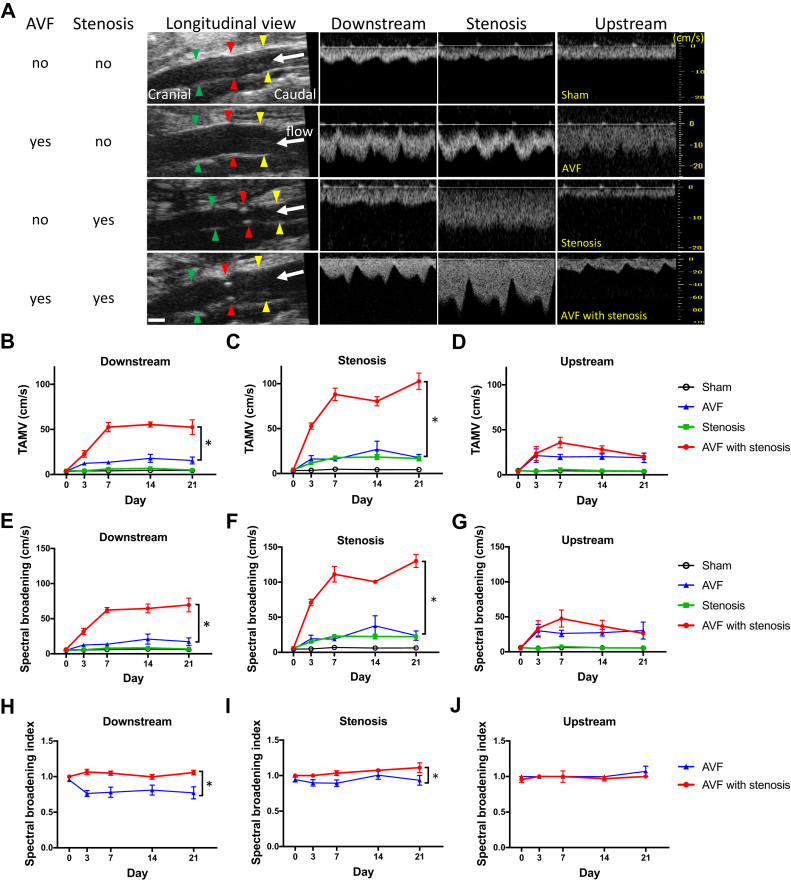
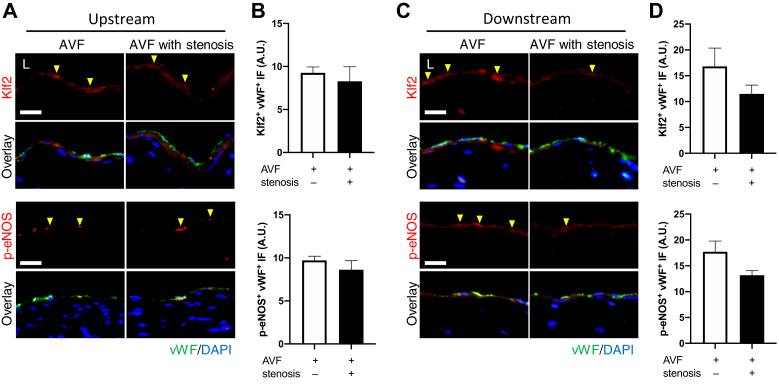
An aortocaval fistula was created between the distal aorta and inferior vena cava (IVC); a stenosis was then created distal to the fistula by partial IVC ligation. Sham-operated animals, AVF without venous stenosis, and venous stenosis without AVF were used as controls. Physiologic properties of the IVC, both upstream and downstream of the stenosis, or the corresponding sites in models without stenosis, were assessed with ultrasound examination on days 0 to 21. The spectral broadening index was measured to assess the degree of disturbed shear stress. The IVC was harvested at day 21 and specimens were analyzed with immunofluorescence.
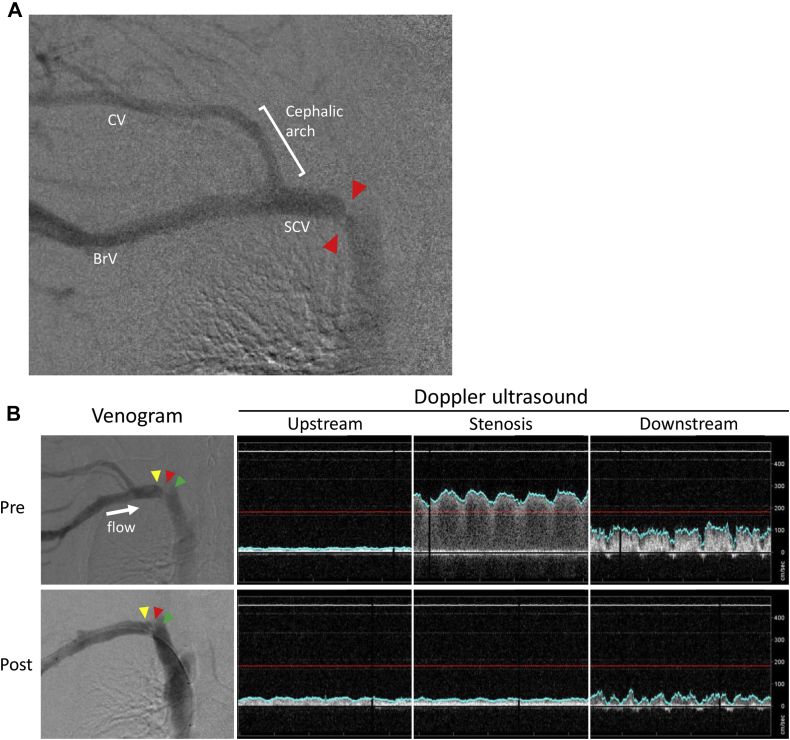
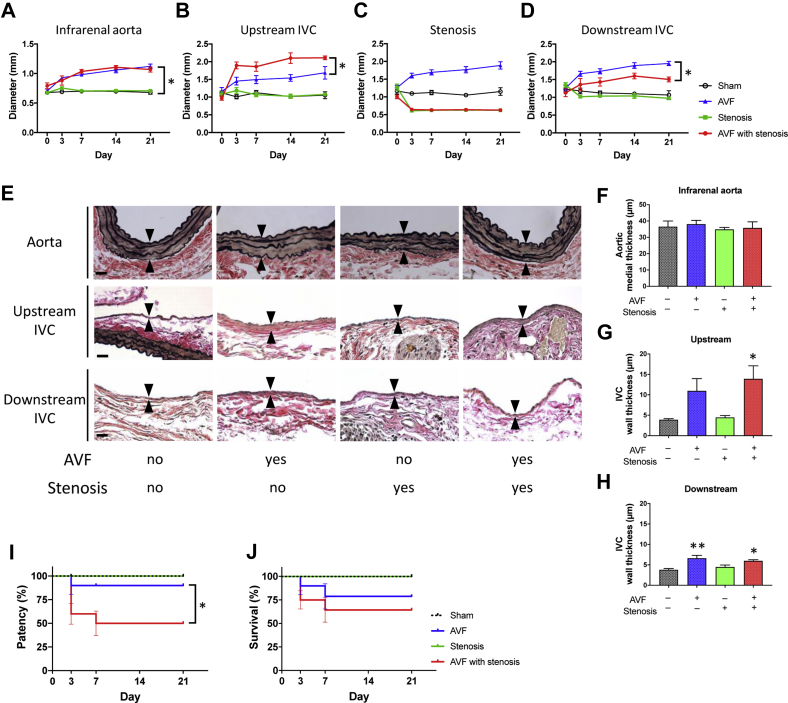
The IVC diameter of mice with an AVF and stenosis showed increased upstream ( = .013), but decreased downstream diameter ( = .001) compared with mice with an AVF but without a stenosis, at all postoperative times (days 3-21). IVC wall thickness increased in mice with an AVF, compared with IVC without an AVF (upstream of stenosis: 13.9 μm vs 11.0 μm vs 4.5 μm vs 3.9 μm; = .020; downstream of stenosis: 6.0 μm vs 6.6 μm vs μm 4.5 μm vs 3.8 μm; = .002; AVF with stenosis, AVF, stenosis, sham, respectively). AVF patency significantly decreased in mice with an AVF and stenosis by day 21 (50% vs 90%; = .048). The IVC of mice with AVF and stenosis showed a venous waveform with pulsatility as well as enhanced velocity at and downstream of the stenosis; similar waveforms were observed in a human case of CVS. Downstream to the stenosis, the spectral broadening index was significantly higher compared with mice with AVF alone (1.06 vs 0.78; = .011; day 21), and there was a trend towards less immunoreactivity of both Krüppel-like factor 2 and phosphorylated-endothelial nitric oxide synthase compared with mice with an AVF alone.
Partial IVC ligation distal to a mouse aortocaval fistula alters the fistula diameter and wall thickness, decreases patency, and increases distal disturbed flow compared with fistulae without a distal stenosis. Our mouse model of stenosis distal to an AVF may be a faithful representation of human CVS that shows similar morphology and physiology, including disturbed shear stress.
中心静脉狭窄(CVS)是动静脉内瘘(AVF)失功的主要原因。然而,传统多普勒超声方法相对难以对中心静脉进行研究。为了解CVS导致AVF失功的潜在机制,建立了一种在AVF远端造成狭窄的动物模型。我们假设该小鼠模型将呈现与人类CVS相似的形态和生理特征。
在远端主动脉和下腔静脉(IVC)之间建立主动脉腔静脉瘘;然后通过部分IVC结扎在瘘远端造成狭窄。假手术动物、无静脉狭窄的AVF以及无AVF的静脉狭窄作为对照。在术后第0至21天,通过超声检查评估狭窄部位上游和下游IVC的生理特性,或无狭窄模型中相应部位的生理特性。测量频谱增宽指数以评估剪切应力紊乱程度。在第21天采集IVC,并用免疫荧光法对标本进行分析。
在所有术后时间点(第3 - 21天),与有AVF但无狭窄的小鼠相比,有AVF和狭窄的小鼠IVC直径在狭窄上游增加(P = 0.013),但在狭窄下游减小(P = 0.001)。与无AVF的IVC相比,有AVF的小鼠IVC壁厚度增加(狭窄上游:13.9μm对11.0μm对4.5μm对3.9μm;P = 0.020;狭窄下游:6.0μm对6.6μm对4.5μm对3.8μm;P = 0.002;分别为有狭窄的AVF、AVF、狭窄、假手术)。到第21天,有AVF和狭窄的小鼠中AVF通畅率显著降低(50%对90%;P = 0.048)。有AVF和狭窄的小鼠IVC在狭窄处及下游呈现出具有搏动性的静脉波形以及流速增加;在1例人类CVS病例中观察到类似波形。与仅有无狭窄AVF的小鼠相比,狭窄下游的频谱增宽指数显著更高(1.06对0.78;P = 0.011;第21天),并且与仅有无狭窄AVF的小鼠相比,Krüppel样因子2和磷酸化内皮型一氧化氮合酶的免疫反应性有降低趋势。
与无远端狭窄的内瘘相比,小鼠主动脉腔静脉瘘远端的部分IVC结扎改变了内瘘直径和壁厚度,降低了通畅率,并增加了远端血流紊乱。我们建立的AVF远端狭窄小鼠模型可能是人类CVS的可靠模型,呈现出相似的形态和生理特征,包括剪切应力紊乱。