Leon H. Charney Division of Cardiology, New York University School of Medicine, NYU Langone Health, 550 1st Avenue, NY, 10016, New York, USA.
J Interv Card Electrophysiol. 2022 Jan;63(1):97-101. doi: 10.1007/s10840-021-00952-w. Epub 2021 Feb 4.
Catheter ablation procedures for atrial fibrillation (AF) were significantly curtailed during the peak of coronavirus disease 2019 (COVID-19) pandemic to conserve healthcare resources and limit exposure. There is little data regarding peri-procedural outcomes of medical procedures during the COVID-19 pandemic. We enacted protocols to safely reboot AF ablation while limiting healthcare resource utilization. We aimed to evaluate acute and subacute outcomes of protocols instituted for reboot of AF ablation during the COVID-19 pandemic.
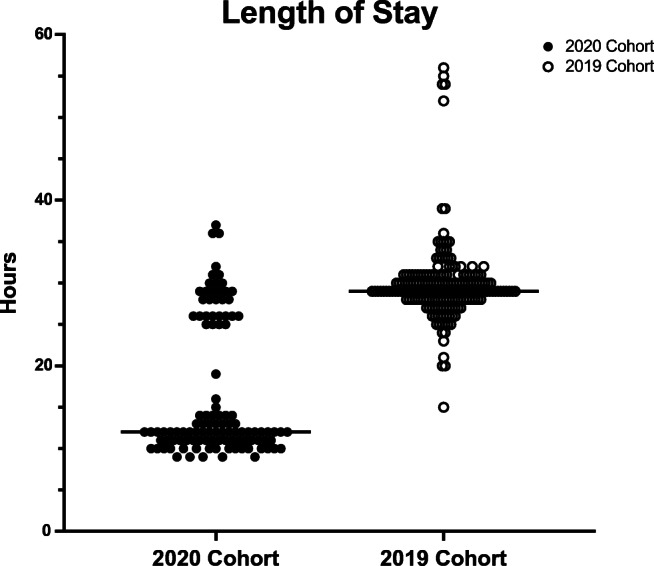
Perioperative healthcare utilization and acute procedural outcomes were analyzed for consecutive patients undergoing AF ablation under COVID-19 protocols (2020 cohort; n=111) and compared to those of patients who underwent AF ablation during the same time period in 2019 (2019 cohort; n=200). Newly implemented practices included preoperative COVID-19 testing, selective transesophageal echocardiography (TEE), utilization of venous closure, and same-day discharge when clinically appropriate.
Pre-ablation COVID-19 testing was positive in 1 of 111 patients. There were 0 cases ablation-related COVID-19 transmission and 0 major complications in either cohort. Pre-procedure TEE was performed in significantly fewer 2020 cohort patients compared to the 2019 cohort patients (68.4% vs. 97.5%, p <0.001, respectively) despite greater prevalence of persistent arrhythmia in the 2020 cohort. Same-day discharge was achieved in 68% of patients in the 2020 cohort, compared to 0% of patients in the 2019 cohort.
Our findings demonstrate the feasibility of safe resumption of complex electrophysiology procedures during the COVID-19 pandemic, reducing healthcare utilization and maintaining quality of care. Protocols instituted may be generalizable to other types of procedures and settings.
为了节省医疗资源并限制暴露,在 2019 年冠状病毒病(COVID-19)大流行高峰期,心房颤动(AF)的导管消融术显著减少。关于 COVID-19 大流行期间医疗程序围手术期结果的数据很少。我们制定了方案,以安全重启 AF 消融,同时限制医疗资源的使用。我们旨在评估 COVID-19 大流行期间为重启 AF 消融而制定的方案的急性和亚急性结果。
分析了在 COVID-19 方案下接受 AF 消融的连续患者(2020 队列;n=111)的围手术期医疗利用情况和急性手术结果,并与同期接受 AF 消融的患者(2019 队列;n=200)进行比较。新实施的做法包括术前 COVID-19 检测、选择性经食管超声心动图(TEE)、静脉闭合的利用以及在临床合适时当天出院。
在 111 名患者中,有 1 名患者的术前 COVID-19 检测呈阳性。在两个队列中均未发生消融相关的 COVID-19 传播,也未发生重大并发症。与 2019 队列相比,2020 队列患者进行术前 TEE 的比例明显较低(分别为 68.4%和 97.5%,p<0.001),尽管 2020 队列患者持续性心律失常的发生率更高。在 2020 队列中,68%的患者实现了当天出院,而在 2019 队列中没有患者当天出院。
我们的研究结果表明,在 COVID-19 大流行期间安全恢复复杂电生理程序是可行的,同时减少了医疗资源的利用并保持了护理质量。制定的方案可能适用于其他类型的程序和环境。