Servicio de Aparato Digestivo, Hospital Universitari de Bellvitge-IDIBELL, Barcelona, España.
Servicio de Aparato Digestivo, Hospital Universitari de Bellvitge-IDIBELL, Barcelona, España.
Gastroenterol Hepatol. 2022 Jan;45(1):9-17. doi: 10.1016/j.gastrohep.2020.11.020. Epub 2021 Feb 2.
The pandemic caused by the SARS-CoV-2 virus has had a serious impact on the functioning of gastrointestinal endoscopy Units. The Asociación Española de Gastroenterología (AEG) and the Sociedad Española de Endoscopia Digestiva (SEED) have proposed the EPAGE guidelines for managing postponed colonoscopies.
To evaluate the EPAGE guidelines as a management tool compared to the immunologic faecal occult blood test (iFOBT) and compared to risk score (RS) that combines age, sex and the iFOBT for the detection of colorectal cancer (CRC) and significant bowel disease (SBD).
A prospective, single-centre study enrolling 743 symptomatic patients referred for a diagnostic colonoscopy. Each order was classified according to the EPAGE guidelines as appropriate, indeterminate or inappropriate. Patients underwent an iFOBT and had their RS calculated.
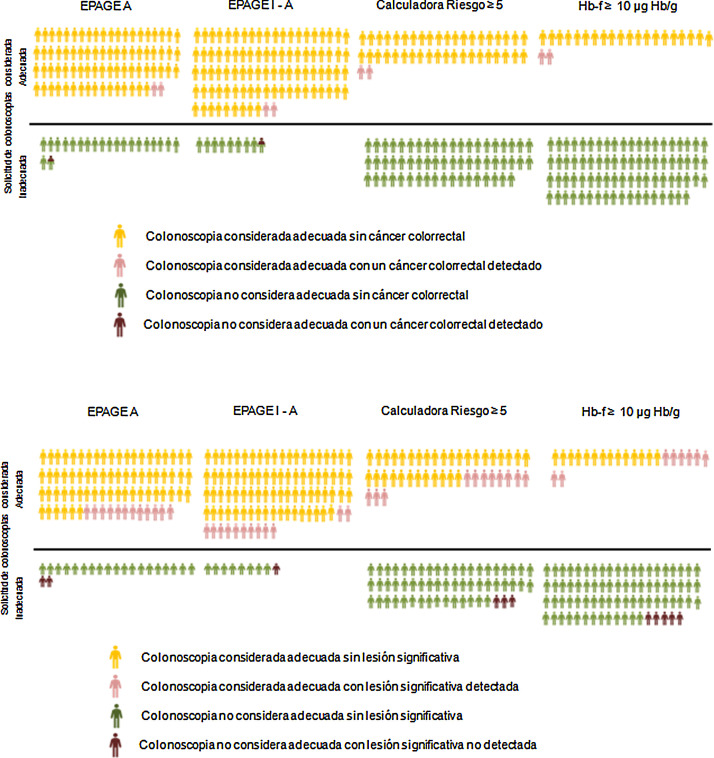
The iFOBT (p<0.001), but not the EPAGE guidelines (p = 0.742), was an independent predictive factor of risk of CRC. The ROC AUCs for the EPAGE guidelines, the iFOBT and the RS were 0.61 (95% CI 0.49-0.75), 0.95 (0.93-0.97) and 0.90 (0.87-0.93) for CRC, and 0.55 (0.49-0.61), 0.75 (0.69-0.813) and 0.78 (0.73-0.83) for SBD, respectively. The numbers of colonoscopies needed to detect a case of CRC and a case of SBD were 38 and seven for the EPAGE guidelines, seven and two for the iFOBT, and 19 and four for a RS ≥5 points, respectively.
The EPAGE guidelines, unlike the iFOBT, is not suitable for screening candidate patients for a diagnostic colonoscopy to detect CRC. The iFOBT, in combination with age and sex, is the most suitable strategy for managing demand for endoscopy in a restricted-access situation.
由 SARS-CoV-2 病毒引起的大流行对胃肠内窥镜检查单位的运作产生了严重影响。西班牙胃肠病学协会(AEG)和西班牙消化内镜学会(SEED)提出了 EPAGE 指南,用于管理推迟的结肠镜检查。
评估 EPAGE 指南作为管理工具,与免疫粪便潜血试验(iFOBT)相比,以及与风险评分(RS)相比,后者结合了年龄、性别和 iFOBT 用于检测结直肠癌(CRC)和显著肠道疾病(SBD)。
一项前瞻性、单中心研究纳入了 743 名因症状就诊接受诊断性结肠镜检查的患者。每个医嘱根据 EPAGE 指南进行适当、不确定或不适当的分类。患者接受 iFOBT 检查并计算 RS。
iFOBT(p<0.001),而不是 EPAGE 指南(p=0.742),是 CRC 风险的独立预测因素。EPAGE 指南、iFOBT 和 RS 的 ROC AUC 分别为 0.61(95%CI 0.49-0.75)、0.95(0.93-0.97)和 0.90(0.87-0.93)用于 CRC,以及 0.55(0.49-0.61)、0.75(0.69-0.813)和 0.78(0.73-0.83)用于 SBD。检测 CRC 和 SBD 病例所需的结肠镜检查数量分别为 38 例和 7 例用于 EPAGE 指南,7 例和 2 例用于 iFOBT,以及 19 例和 4 例用于 RS≥5 分。
与 iFOBT 不同,EPAGE 指南不适合筛选接受诊断性结肠镜检查以检测 CRC 的候选患者。iFOBT 结合年龄和性别是在受限情况下管理内镜需求的最适合策略。