Makurumidze Richard, Gombe Notion Tafara, Magure Tapuwa, Tshimanga Mufuta
Department of Community Medicine, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe.
National AIDS Council, Harare, Zimbabwe.
BMC Public Health. 2021 Feb 5;21(1):298. doi: 10.1186/s12889-021-10275-0.
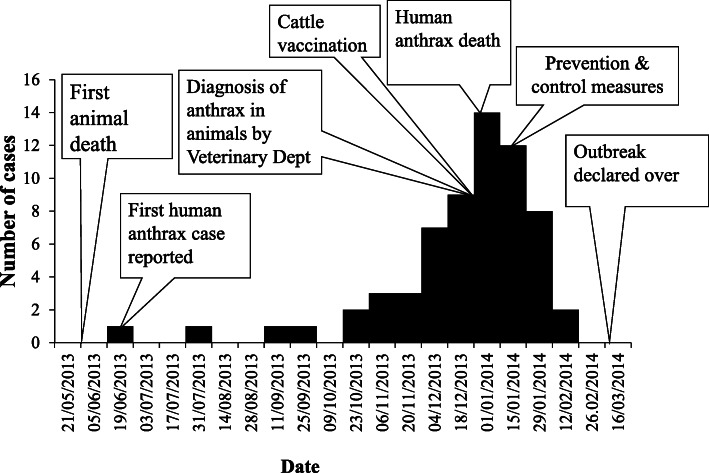
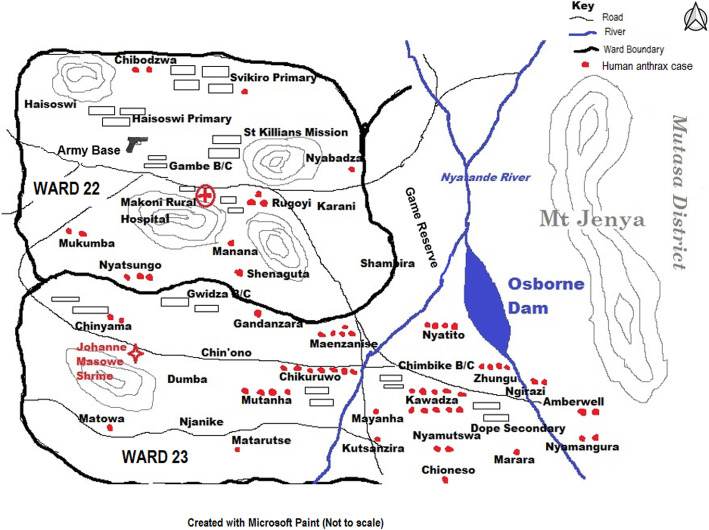
Anthrax continues to be a disease of public health importance in Zimbabwe, with sporadic outbreaks reported annually in many parts of the country. A human anthrax outbreak occurred in wards 22 and 23 of Makoni District from mid-June 2013 to end of January 2014, following cattle deaths in the wards. Laboratory tests confirmed anthrax as the cause for the cattle deaths. This study investigated the clinical characteristics, distribution of cases (places, person and time) and risk factors for contracting the anthrax disease. We also assessed the environment, district preparedness and response, and outbreak prevention and control measures.
We conducted an outbreak investigation using a mixed-methods design. A 1:1 case-control study was used to assess risk factors for contracting anthrax. The controls were frequency matched to cases by sex. Data were collected using a structured interviewer-administered questionnaire. Environmental assessment, district preparedness and response, and outbreak prevention and control measures were assessed using a checklist, observations, and key informant interviews. Multivariable unconditional logic regression analysis was performed to identify independent risk factors associated with contracting anthrax.
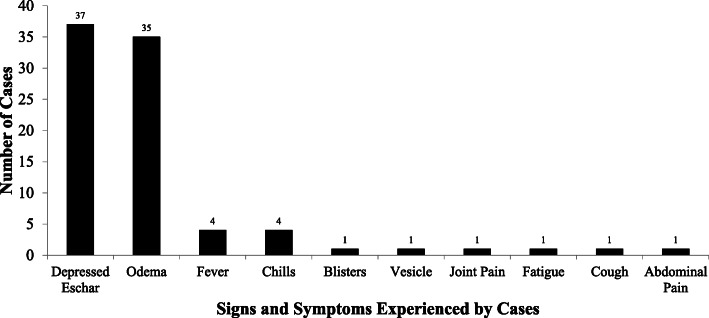
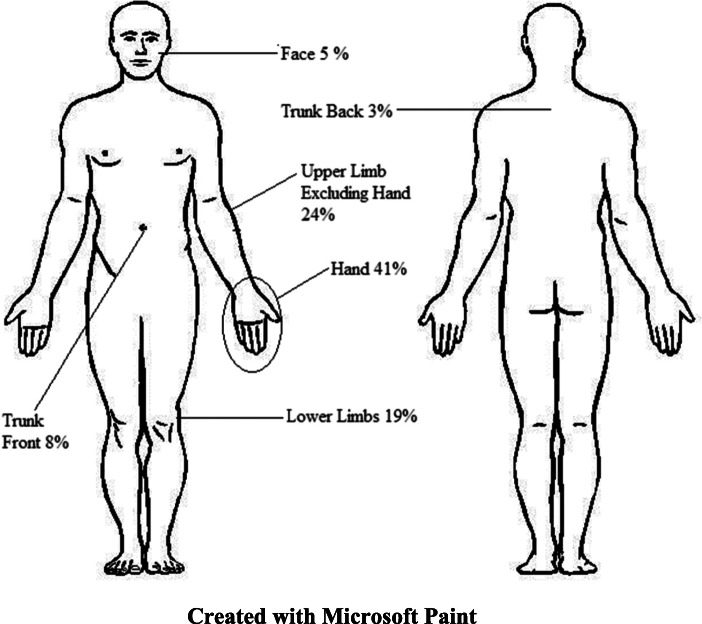
We interviewed 37 of the 64 cases, along with 37 controls. All the cases had cutaneous anthrax, with the hand being the most common site of the eschar (43%). Most of the cases (89%) were managed according to the national guidelines. Multivariable analysis demonstrated that meat sourced from other villages [vs butchery, OR = 15.21, 95% CI (2.32-99.81)], skinning [OR = 4.32, 95% CI (1.25-14.94)], and belonging to religions that permit eating meat from cattle killed due to unknown causes or butchered after unobserved death [OR = 6.12, 95% CI (1.28-29.37)] were associated with contracting anthrax. The poor availability of resources in the district caused a delayed response to the outbreak.
The described anthrax outbreak was caused due to contact with infected cattle meat. Although the outbreak was eventually controlled through cattle vaccination and health education and awareness campaigns, the response of the district office was initially delayed and insufficient. The district should strengthen its emergency preparedness and response capacity, revive zoonotic committees, conduct awareness campaigns and improve surveillance, especially during outbreak seasons.
在津巴布韦,炭疽仍然是一种具有公共卫生重要性的疾病,该国许多地区每年都有散发病例报告。2013年6月中旬至2014年1月底,马科尼区第22和23病房发生了一起人类炭疽疫情,此前这些病房出现了牛死亡情况。实验室检测证实炭疽是牛死亡的原因。本研究调查了炭疽病的临床特征、病例分布(地点、人员和时间)以及感染炭疽病的风险因素。我们还评估了环境、地区的准备和应对情况以及疫情防控措施。
我们采用混合方法设计进行了一次疫情调查。采用1:1病例对照研究来评估感染炭疽的风险因素。对照组按性别与病例进行频率匹配。通过结构化访谈问卷收集数据。使用清单、观察和关键信息访谈对环境评估、地区准备和应对情况以及疫情防控措施进行评估。进行多变量无条件逻辑回归分析以确定与感染炭疽相关的独立风险因素。
我们对64例病例中的37例以及37名对照进行了访谈。所有病例均为皮肤炭疽,手部是焦痂最常见的部位(43%)。大多数病例(89%)按照国家指南进行了治疗。多变量分析表明,来自其他村庄的肉类[与屠宰场相比,比值比(OR)=15.21,95%置信区间(CI)(2.32 - 99.81)]、剥皮[OR = 4.32,95% CI(1.25 - 14.94)]以及属于允许食用因不明原因死亡或在未观察到死亡后屠宰的牛的肉类的宗教群体[OR = 6.12,95% CI(1.28 - 29.37)]与感染炭疽有关。该地区资源匮乏导致对疫情的应对延迟。
所述炭疽疫情是由于接触受感染的牛肉引起的。尽管最终通过牛疫苗接种以及健康教育和宣传活动控制了疫情,但地区办公室的应对最初出现延迟且力度不足。该地区应加强其应急准备和应对能力,恢复人畜共患病委员会,开展宣传活动并加强监测,尤其是在疫情高发季节。