Department of Dermatology, Ann & Robert H. Lurie Children's Hospital of Chicago, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Department of Pediatric Allergy & Immunology, Ann & Robert H. Lurie Children's Hospital of Chicago, Northwestern University Feinberg School of Medicine, Chicago, Illinois.
Ann Allergy Asthma Immunol. 2021 May;126(5):562-568.e1. doi: 10.1016/j.anai.2021.01.027. Epub 2021 Feb 4.
Little is known on the clinical manifestations of coconut allergy. Our knowledge to date is mainly based on case reports.
To characterize the allergic reactions to coconut and suggest diagnostic cutoffs for specific immunoglobulin E (sIgE) and skin prick testing (SPT) to predict clinically reactive coconut allergy.
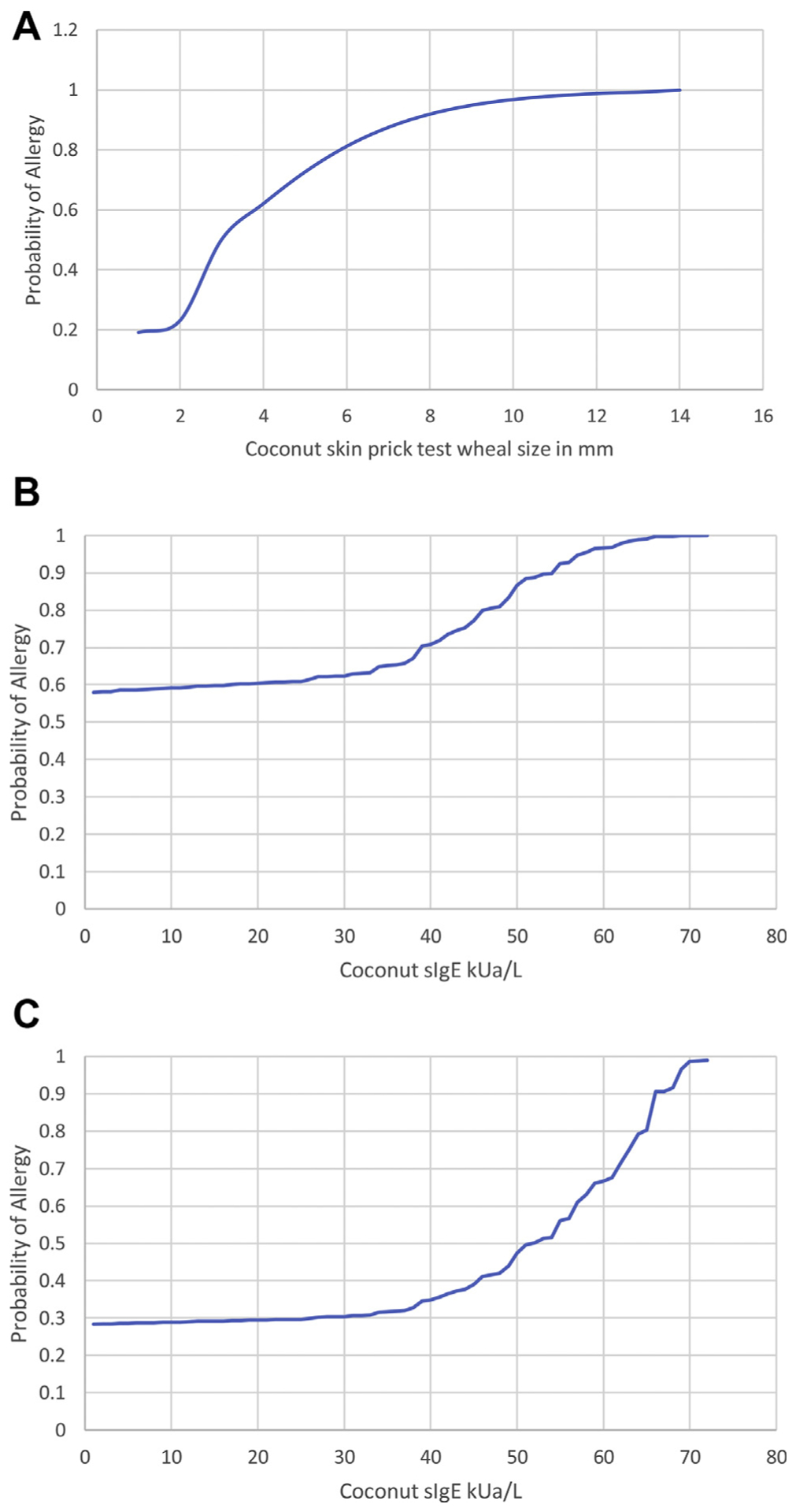
Methods include retrospective chart review at an urban tertiary care center of patients with positive testing result for coconut. Probability curves were computed by logistic regression for SPT and coconut sIgE.
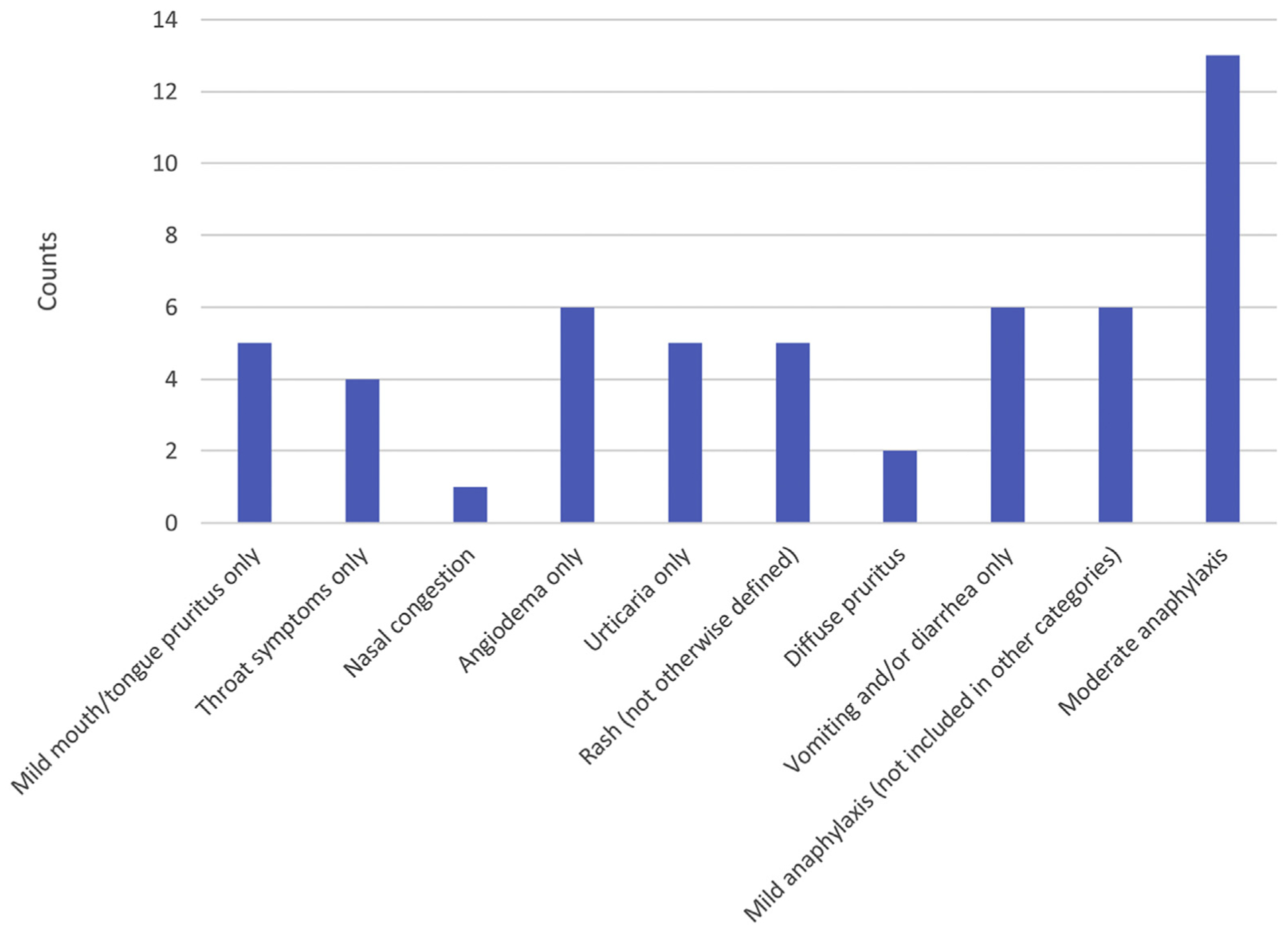
Of 275 records reviewed, 69 patients reported coconut reactions and 206 were sensitized only or nonallergic. The reactions occurred with breastfeeding (n = 2), contact (n = 10), or oral ingestion (n = 57). Approximately 50% of oral ingestion reactions were associated with mild/moderate anaphylaxis. Clinical reactivity vs sensitization was more common in topical coconut users (2-fold) (P = .02). Although not statistically significant, there was a trend toward more coconut allergy vs sensitization in Asian and African American patients. The probability of allergy with positive SPT result was approximately 50% and with sIgE was approximately 60%. At an SPT of 9 mm wheal or sIgE of 58 kU of allergen/L, there is a 95% probability of reaction. Cosensitization with tree nuts, legumes, and seeds was common. Macadamia nut had the strongest correlation with coconut (r = 0.81, P < .001, n = 101).
Although the rate of reactivity to coconut in sensitized individuals is low, half of the reactions from consumption met the criteria for anaphylaxis. Clinicians should be aware of the spectrum of reactions and diagnostic use of sIgE and SPT.
对椰子过敏的临床表现知之甚少。我们目前的知识主要基于病例报告。
描述椰子过敏的过敏反应,并提出用于特异性免疫球蛋白 E(sIgE)和皮肤点刺试验(SPT)的诊断截止值,以预测临床上有反应的椰子过敏。
方法包括在城市三级保健中心对椰子检测结果阳性的患者进行回顾性图表审查。通过逻辑回归计算 SPT 和椰子 sIgE 的概率曲线。
在审查的 275 份记录中,有 69 份报告了椰子过敏反应,206 份仅为致敏或非过敏。反应发生在母乳喂养时(n=2)、接触时(n=10)或口服摄入时(n=57)。大约 50%的口服摄入反应与轻度/中度过敏反应有关。与致敏相比,局部使用椰子的患者更常见临床反应(2 倍)(P=0.02)。尽管没有统计学意义,但在亚洲和非裔美国患者中,椰子过敏与致敏相比有增加的趋势。阳性 SPT 结果的过敏概率约为 50%,sIgE 约为 60%。SPT 为 9 毫米风团或 sIgE 为 58 kU/L 时,发生反应的概率为 95%。与树坚果、豆类和种子的共同致敏很常见。澳洲坚果与椰子的相关性最强(r=0.81,P<0.001,n=101)。
尽管致敏个体对椰子的反应率较低,但一半的消费反应符合过敏反应的标准。临床医生应了解反应谱和 sIgE 和 SPT 的诊断用途。