Division of Pharmacodynamics, Keio University Faculty of Pharmacy, 1-5-30 Shibakoen, Minato-ku, Tokyo, 105-8512, Japan.
Department of Pharmacy, Kumamoto University Hospital, 1-1-1, Honjo, Chuo-ku, Kumamoto-shi, Kumamoto, 860-8556, Japan.
BMC Infect Dis. 2021 Feb 6;21(1):153. doi: 10.1186/s12879-021-05858-6.
This systematic review and meta-analysis explored the relationship between vancomycin (VCM) monitoring strategies and VCM effectiveness and safety.
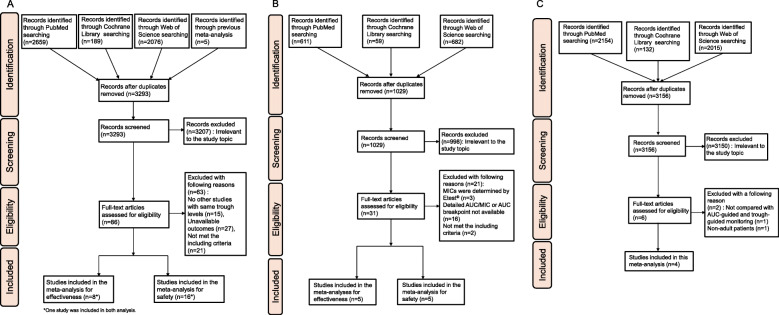
We conducted our analysis using the MEDLINE, Web of Sciences, and Cochrane Register of Controlled Trials electronic databases searched on August 9, 2020. We calculated odds ratios (ORs) and 95% confidence intervals (CIs).
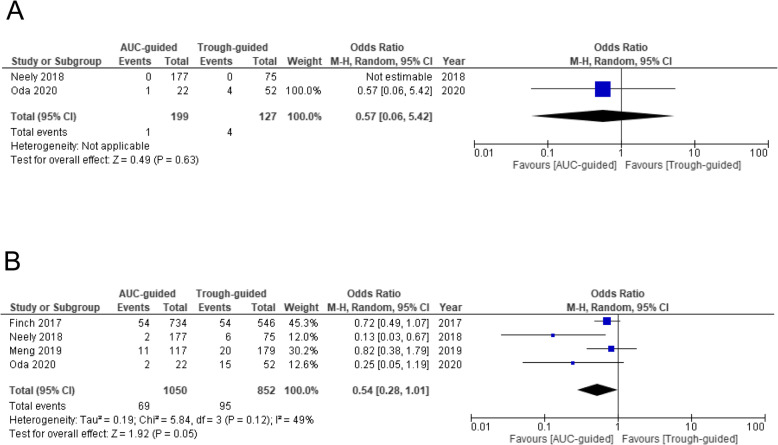
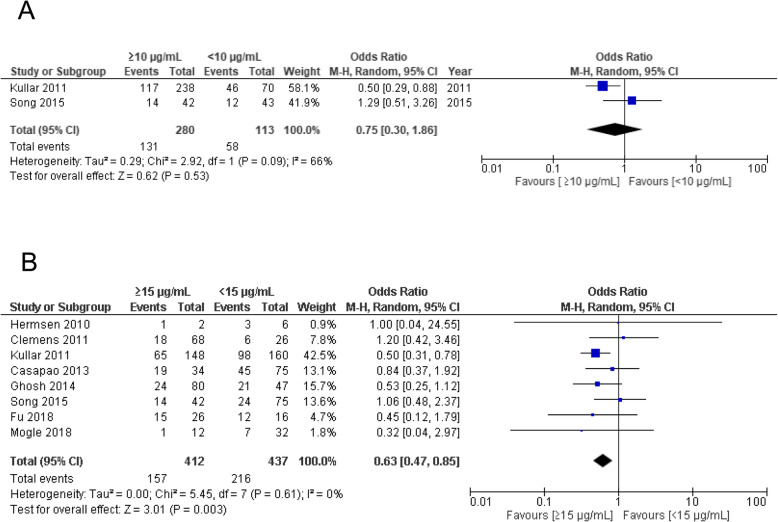
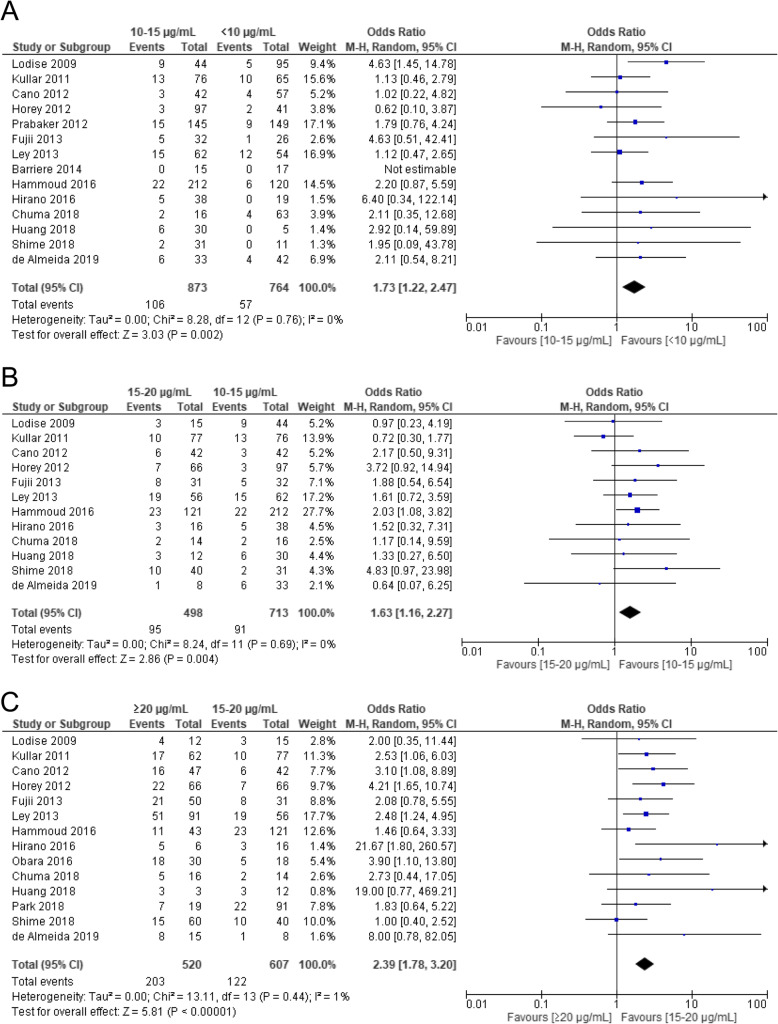
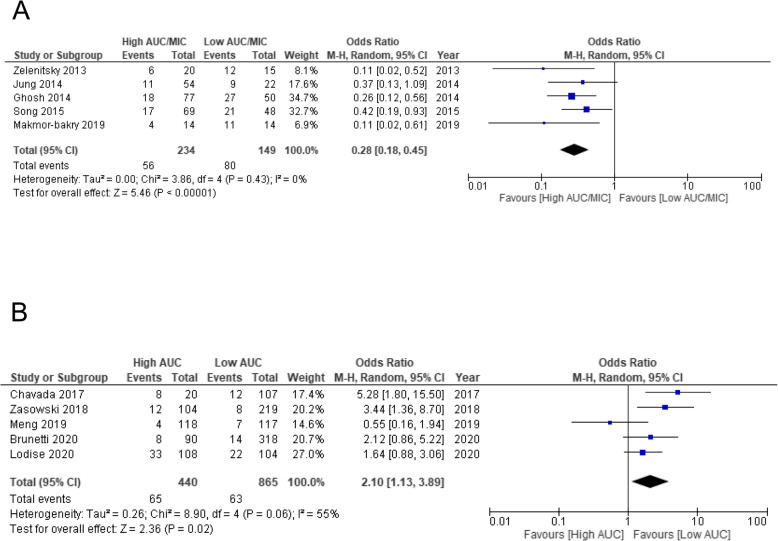
Adult patients with methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia with VCM trough concentrations ≥15 μg/mL had significantly lower treatment failure rates (OR 0.63, 95% CI 0.47-0.85). The incidence of acute kidney injury (AKI) increased with increased trough concentrations and was significantly higher for trough concentrations ≥20 μg/mL compared to those at 15-20 μg/mL (OR 2.39, 95% CI 1.78-3.20). Analysis of the target area under the curve/minimum inhibitory concentration ratios (AUC/MIC) showed significantly lower treatment failure rates for high AUC/MIC (cut-off 400 ± 15%) (OR 0.28, 95% CI 0.18-0.45). The safety analysis revealed that high AUC value (cut-off 600 ± 15%) significantly increased the risk of AKI (OR 2.10, 95% CI 1.13-3.89). Our meta-analysis of differences in monitoring strategies included four studies. The incidence of AKI tended to be lower in AUC-guided monitoring than in trough-guided monitoring (OR 0.54, 95% CI 0.28-1.01); however, it was not significant in the analysis of mortality.
We identified VCM trough concentrations and AUC values that correlated with effectiveness and safety. Furthermore, compared to trough-guided monitoring, AUC-guided monitoring showed potential for decreasing nephrotoxicity.
本系统评价和荟萃分析探讨了万古霉素(VCM)监测策略与 VCM 有效性和安全性之间的关系。
我们于 2020 年 8 月 9 日检索了 MEDLINE、Web of Sciences 和 Cochrane 对照试验注册库电子数据库,进行了分析。我们计算了比值比(OR)和 95%置信区间(CI)。
万古霉素谷浓度≥15μg/mL 的耐甲氧西林金黄色葡萄球菌(MRSA)菌血症成年患者治疗失败率显著降低(OR 0.63,95%CI 0.47-0.85)。急性肾损伤(AKI)的发生率随谷浓度的增加而增加,且谷浓度≥20μg/mL 者显著高于 15-20μg/mL 者(OR 2.39,95%CI 1.78-3.20)。目标 AUC/MIC 比值的分析显示,高 AUC/MIC(切点 400±15%)的治疗失败率显著降低(OR 0.28,95%CI 0.18-0.45)。安全性分析显示,高 AUC 值(切点 600±15%)显著增加 AKI 的风险(OR 2.10,95%CI 1.13-3.89)。我们对监测策略差异的荟萃分析包括四项研究。与谷浓度监测相比,AUC 监测的 AKI 发生率有降低趋势(OR 0.54,95%CI 0.28-1.01);但在死亡率分析中无统计学意义。
我们确定了与有效性和安全性相关的万古霉素谷浓度和 AUC 值。此外,与谷浓度监测相比,AUC 监测可能降低肾毒性。