Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, New Jersey, USA.
Touro College of Pharmacy, New York, New York, USA.
Pharmacotherapy. 2022 Sep;42(9):741-753. doi: 10.1002/phar.2722. Epub 2022 Aug 5.
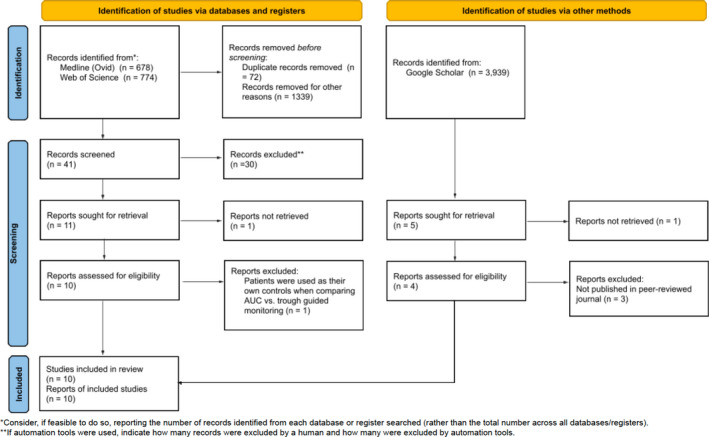
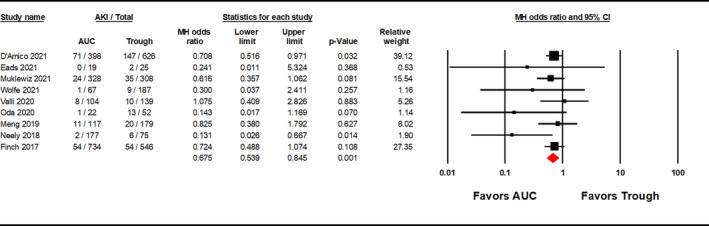
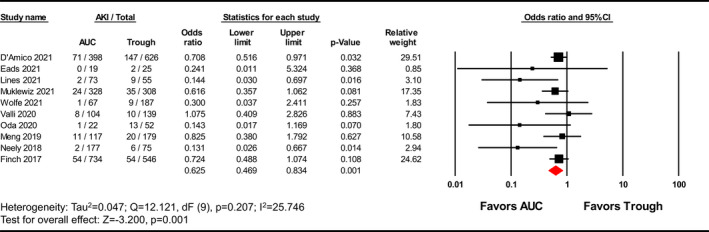
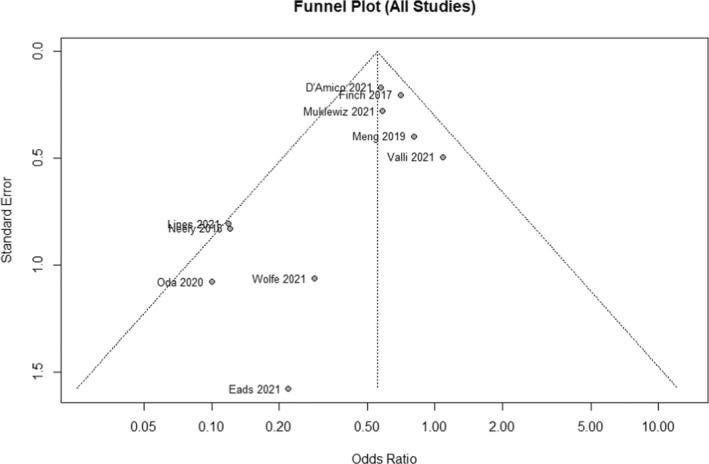
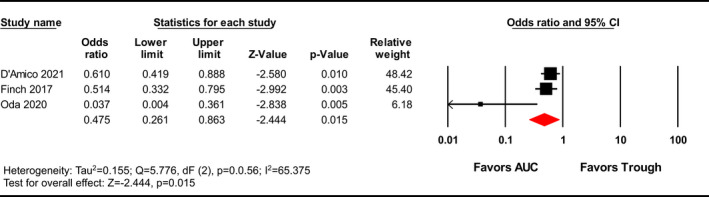
Vancomycin is commonly used to treat methicillin-resistant Staphylococcus aureus infections and is known to cause nephrotoxicity. Previous Vancomycin Consensus Guidelines recommended targeting trough concentrations but the 2020 Guidelines suggest monitoring vancomycin area under the curve (AUC) given the reduced risk of acute kidney injury (AKI) at similar levels of efficacy. This meta-analysis compares vancomycin-induced AKI incidence using AUC-guided dosing strategies versus trough-based monitoring. Literature was queried from Medline (Ovid), Web of Science, and Google Scholar from database inception through November 5, 2021. Interventional or observational studies reporting the incidence of vancomycin-induced AKI between AUC- and trough-guided dosing strategies were included. In the primary analysis, the Vancomycin Consensus Guidelines definition for AKI was used if reported; otherwise, the Risk, Injury, and Failure; and Loss, and End-stage kidney disease (RIFLE) or Kidney Disease Improving Global Outcomes (KDIGO) definitions were used. The incidence of nephrotoxicity was evaluated between the two strategies using a Mantel-Haenszel random-effects model, and odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Subgroup analyses for adjusted ORs and AKI definitions were performed. Heterogeneity was identified using Cochrane's Q test and I statistics. A total of 10 studies with 4231 patients were included. AUC-guided dosing strategies were associated with significantly less vancomycin-induced AKI than trough-guided strategies [OR 0.625, 95% CI (0.469-0.834), p = 0.001; I = 25.476]. A subgroup analysis of three studies reporting adjusted ORs yielded similar results [OR 0.475, 95% CI (0.261-0.863), p = 0.015]. Stratification by AKI definition showed a significant reduction in AKI with the Vancomycin Consensus Guidelines definition [OR 0.552, 95% CI (0.341-0.894), p = 0.016] but failed to find significance in the alternative definitions. Area under the curve-guided dosing strategies are associated with a lower incidence of vancomycin-induced AKI versus trough-guided dosing strategies (GRADE, low). Limitations included the variety of AKI definitions and the potential for confounding bias.
万古霉素常用于治疗耐甲氧西林金黄色葡萄球菌感染,已知其具有肾毒性。以前的万古霉素共识指南建议靶向谷浓度,但 2020 年指南建议监测万古霉素 AUC,因为在类似疗效水平下,急性肾损伤 (AKI) 的风险降低。这项荟萃分析比较了 AUC 指导剂量策略与基于谷浓度监测的万古霉素诱导 AKI 的发生率。文献检索来自 Medline (Ovid)、Web of Science 和 Google Scholar,从数据库建立到 2021 年 11 月 5 日。纳入了报告 AUC 指导剂量策略与谷浓度指导剂量策略之间万古霉素诱导 AKI 发生率的干预性或观察性研究。在主要分析中,如果报告了 AKI,则使用万古霉素共识指南的 AKI 定义;否则,使用风险、损伤和衰竭;以及失代偿期和终末期肾病 (RIFLE) 或改善全球肾脏病结局组织 (KDIGO) 定义。使用 Mantel-Haenszel 随机效应模型评估两种策略之间的肾毒性发生率,并计算比值比 (OR) 和 95%置信区间 (CI)。进行了调整后的 OR 和 AKI 定义的亚组分析。使用 Cochrane Q 检验和 I 统计量确定异质性。共纳入 10 项研究,共 4231 例患者。AUC 指导剂量策略与谷浓度指导剂量策略相比,万古霉素诱导 AKI 的发生率显著降低 [OR 0.625,95%CI (0.469-0.834),p = 0.001;I 25.476]。对三项报告调整后的 OR 的研究进行的亚组分析得出了类似的结果 [OR 0.475,95%CI (0.261-0.863),p = 0.015]。根据 AKI 定义分层显示,使用万古霉素共识指南定义,AKI 显著减少 [OR 0.552,95%CI (0.341-0.894),p = 0.016],但在替代定义中未发现显著性。AUC 指导剂量策略与谷浓度指导剂量策略相比,万古霉素诱导 AKI 的发生率较低 (GRADE,低)。局限性包括 AKI 定义的多样性和潜在的混杂偏倚。