Abe Temidayo, Eyituoyo Harry Onoriode, De Allie Gabrielle, Olanipekun Titilope, Effoe Valery Sammah, Olaosebikan Kikelomo, Mather Paul
Department of Internal Medicine, Morehouse School of Medicine, Atlanta, GA 30310, United States.
Department of Internal Medicine, Mercer University School of Medicine, Macon, GA 31207, United States.
World J Cardiol. 2021 Jan 26;13(1):11-20. doi: 10.4330/wjc.v13.i1.11.
There is a lack of data on the clinical outcomes in patients with native valve infective endocarditis (NVIE) and diabetes mellitus (DM).
To investigate (1) trends in the prevalence of DM among patients with NVIE; and (2) the impact of DM on NVIE outcomes.
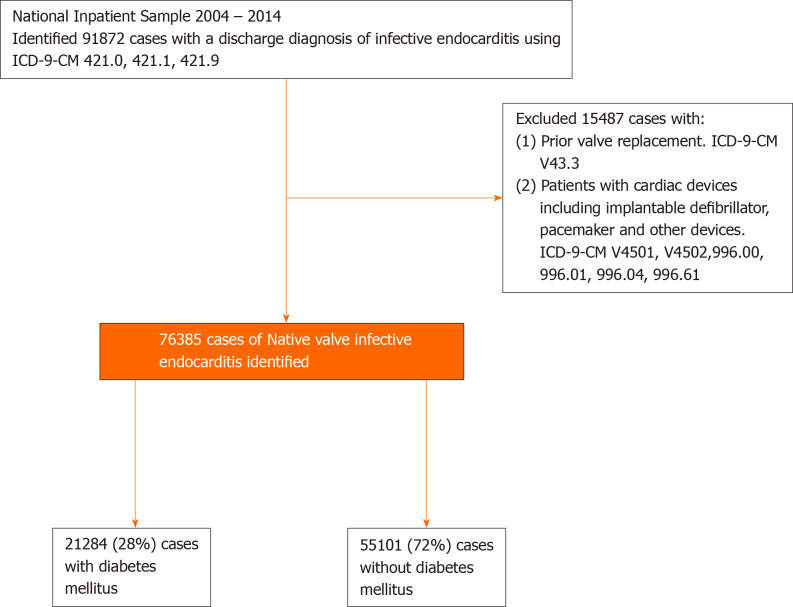
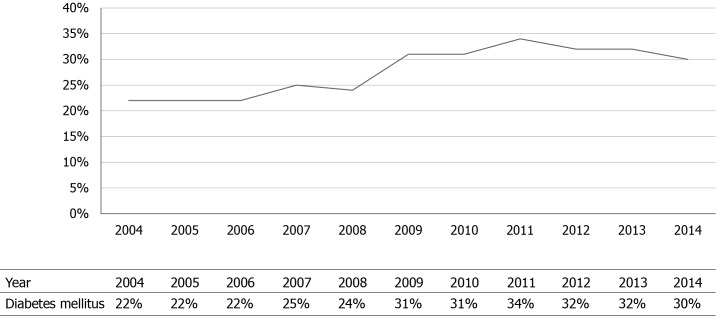
We identified 76385 with NVIE from the 2004 to 2014 National Inpatient Sample, of which 22284 (28%) had DM. We assessed trends in DM from 2004 to 2014 using the Cochrane Armitage test. We compared baseline comorbidities, microorganisms, and in-patients procedures between those with without DM. Propensity match analysis and multivariate logistic regression were used to investigate study outcomes in in-hospital mortality, stroke, acute heart failure, cardiogenic shock, septic shock, and atrioventricular block.
Crude rates of DM increased from in 22% in 2004 to 30% in 2014. There were significant differences in demographics, comorbidities and NVIE risk factors between the two groups. Staphylococcus aureus was the most common organism identified with higher rates in patients with DM (33.1% 35.6%; < 0.0001). After propensity matching, in-hospital mortality (11.1% 11.9%; < 0.0001), stroke (2.3% 3.0%; < 0.0001), acute heart failure (4.6% 6.5%; = 0.001), cardiogenic shock (1.5% 1.9%; < 0.0001), septic shock (7.2% 9.6%; < 0.0001), and atrioventricular block (1.5% 2.4%; < 0.0001), were significantly higher in patients with DM. Independent predictors of mortality in NVIE patients with DM include hemodialysis, congestive heart failure, atrial fibrillation, staphylococcus aureus, and older age.
There is an increasing prevalence of DM in NVIE and it is associated with poorer outcomes. Further studies are crucial to identify the clinical, and sociodemographic contributors to this trend and develop strategies to mitigate its attendant risk.
关于天然瓣膜感染性心内膜炎(NVIE)合并糖尿病(DM)患者的临床结局数据匮乏。
调查(1)NVIE患者中DM的患病率趋势;(2)DM对NVIE结局的影响。
我们从2004年至2014年全国住院患者样本中识别出76385例NVIE患者,其中22284例(28%)患有DM。我们使用Cochrane-Armitage检验评估2004年至2014年期间DM的趋势。我们比较了有DM和无DM患者的基线合并症、微生物及住院治疗情况。倾向匹配分析和多因素逻辑回归用于研究住院死亡率、中风、急性心力衰竭、心源性休克、感染性休克和房室传导阻滞的研究结局。
DM的粗发病率从2004年的22%增至2014年的30%。两组在人口统计学、合并症及NVIE危险因素方面存在显著差异。金黄色葡萄球菌是最常见的病原体,DM患者中的发生率更高(分别为33.1%和35.6%;P<0.0001)。倾向匹配后,DM患者的住院死亡率(分别为11.1%和11.9%;P<0.0001)、中风(分别为2.3%和3.0%;P<0.0001)、急性心力衰竭(分别为4.6%和6.5%;P=0.001)、心源性休克(分别为1.5%和1.9%;P<0.0001)、感染性休克(分别为7.2%和9.6%;P<0.0001)和房室传导阻滞(分别为1.5%和2.4%;P<0.0001)均显著更高。DM的NVIE患者死亡的独立预测因素包括血液透析、充血性心力衰竭、心房颤动、金黄色葡萄球菌感染及高龄。
NVIE患者中DM的患病率呈上升趋势,且与较差的结局相关。进一步研究对于确定导致这一趋势的临床及社会人口学因素并制定降低相关风险的策略至关重要。