Baluku Joseph Baruch, Nakazibwe Bridget, Naloka Joshua, Nabwana Martin, Mwanja Sarah, Mulwana Rose, Sempiira Mike, Nassozi Sylvia, Babirye Febronius, Namugenyi Carol, Ntambi Samuel, Namiiro Sharon, Bongomin Felix, Katuramu Richard, Andia-Biraro Irene, Worodria William
Division of Pulmonology, Mulago National Referral Hospital, Kampala, Uganda.
Mildmay Uganda, Wakiso, Uganda.
J Clin Tuberc Other Mycobact Dis. 2021 Jan 27;23:100221. doi: 10.1016/j.jctube.2021.100221. eCollection 2021 May.
Comorbid conditions and adverse drug events are associated with poor treatment outcomes among patients with drug resistant tuberculosis (DR - TB). This study aimed at determining the treatment outcomes of DR - TB patients with poor prognostic indicators in Uganda.
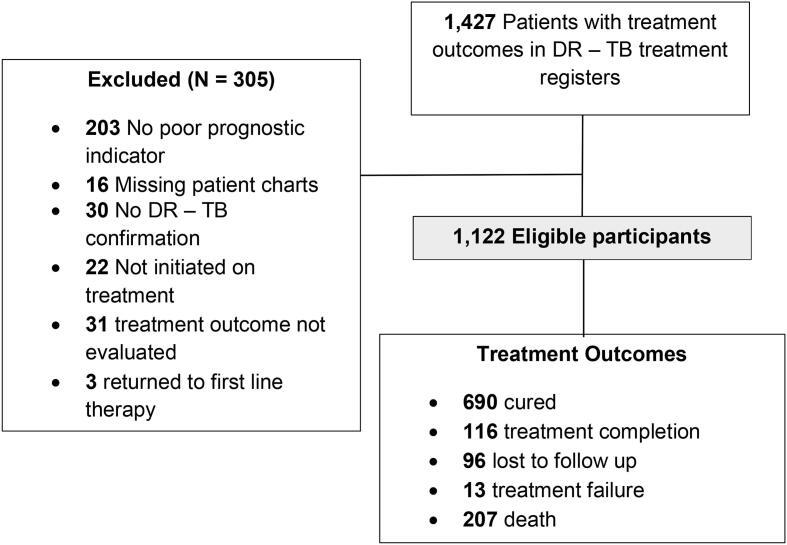
We reviewed treatment records of DR - TB patients from 16 treatment sites in Uganda. Eligible patients had confirmed DR - TB, a treatment outcome in 2014-2019 and at least one of 15 pre-defined poor prognostic indicators at treatment initiation or during therapy. The pre-defined poor prognostic indicators were HIV co-infection, diabetes, heart failure, malignancy, psychiatric illness/symptoms, severe anaemia, alcohol use, cigarette smoking, low body mass index, elevated creatinine, hepatic dysfunction, hearing loss, resistance to fluoroquinolones and/or second-line aminoglycosides, previous exposure to second-line drugs (SLDs), and pregnancy. Tuberculosis treatment outcomes were treatment success, mortality, loss to follow up, and treatment failure as defined by the World Health Organisation. We used logistic and cox proportional hazards regression analysis to determine predictors of treatment success and mortality, respectively.
Of 1122 DR - TB patients, 709 (63.2%) were male and the median (interquartile range, IQR) age was 36.0 (28.0-45.0) years. A total of 925 (82.4%) had ≥2 poor prognostic indicators. Treatment success and mortality occurred among 806 (71.8%) and 207 (18.4%) patients whereas treatment loss-to-follow-up and failure were observed among 96 (8.6%) and 13 (1.2%) patients, respectively. Mild (OR: 0.57, 95% CI 0.39-0.84, p = 0.004), moderate (OR: 0.18, 95% CI 0.12-0.26, p < 0.001) and severe anaemia (OR: 0.09, 95% CI 0.05-0.17, p < 0.001) and previous exposure to SLDs (OR: 0.19, 95% CI 0.08-0.48, p < 0.001) predicted lower odds of treatment success while the number of poor prognostic indicators (HR: 1.62, 95% CI 1.30-2.01, p < 0.001), for every additional poor prognostic indicator) predicted mortality.
Among DR - TB patients with multiple poor prognostic indicators, mortality was the most frequent unsuccessful outcomes. Every additional poor prognostic indicator increased the risk of mortality while anaemia and previous exposure to SLDs were associated with lower odds of treatment success. The management of anaemia among DR - TB patients needs to be evaluated by prospective studies. DR - TB programs should also optimise DR - TB treatment the first time it is initiated.
合并症和药物不良事件与耐多药结核病(DR-TB)患者的治疗效果不佳相关。本研究旨在确定乌干达具有不良预后指标的耐多药结核病患者的治疗效果。
我们回顾了乌干达16个治疗点的耐多药结核病患者的治疗记录。符合条件的患者确诊为耐多药结核病,有2014年至2019年的治疗结果,且在治疗开始时或治疗期间具有15项预先定义的不良预后指标中的至少一项。预先定义的不良预后指标包括艾滋病毒合并感染、糖尿病、心力衰竭、恶性肿瘤、精神疾病/症状、严重贫血、饮酒、吸烟、低体重指数、肌酐升高、肝功能障碍、听力丧失、对氟喹诺酮类和/或二线氨基糖苷类耐药、既往接触过二线药物(SLDs)以及妊娠。结核病治疗结果按照世界卫生组织的定义分为治疗成功、死亡、失访和治疗失败。我们分别使用逻辑回归和Cox比例风险回归分析来确定治疗成功和死亡的预测因素。
在1122例耐多药结核病患者中,709例(63.2%)为男性,年龄中位数(四分位间距,IQR)为36.0(28.0 - 45.0)岁。共有925例(82.4%)患者具有≥2项不良预后指标。806例(71.8%)患者治疗成功,207例(18.4%)患者死亡,96例(8.6%)患者失访,13例(1.2%)患者治疗失败。轻度(比值比:0.57,95%置信区间0.39 - 0.84,p = 0.004)、中度(比值比:0.18,95%置信区间0.12 - 0.26,p < 0.001)和重度贫血(比值比:0.09,95%置信区间0.05 - 0.17,p < 0.001)以及既往接触过二线药物(比值比:0.19,95%置信区间0.08 - 0.48,p < 0.001)预示治疗成功的几率较低,而不良预后指标的数量(风险比:1.62,95%置信区间1.30 - 2.01,p < 0.001,每增加一项不良预后指标)预示死亡风险。
在具有多项不良预后指标的耐多药结核病患者中,死亡是最常见的治疗失败结局。每增加一项不良预后指标,死亡风险就会增加,而贫血和既往接触过二线药物与治疗成功几率较低相关。需要通过前瞻性研究评估耐多药结核病患者贫血的管理。耐多药结核病项目还应在首次启动时优化耐多药结核病治疗。