Digestive Disease SectionInternal MedicineYale School of MedicineNew HavenCTUSA.
VA-Connecticut Healthcare SystemWest HavenCTUSA.
Hepatol Commun. 2020 Dec 12;5(2):272-282. doi: 10.1002/hep4.1641. eCollection 2021 Feb.
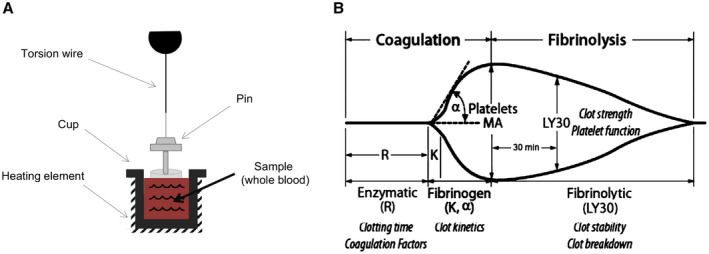
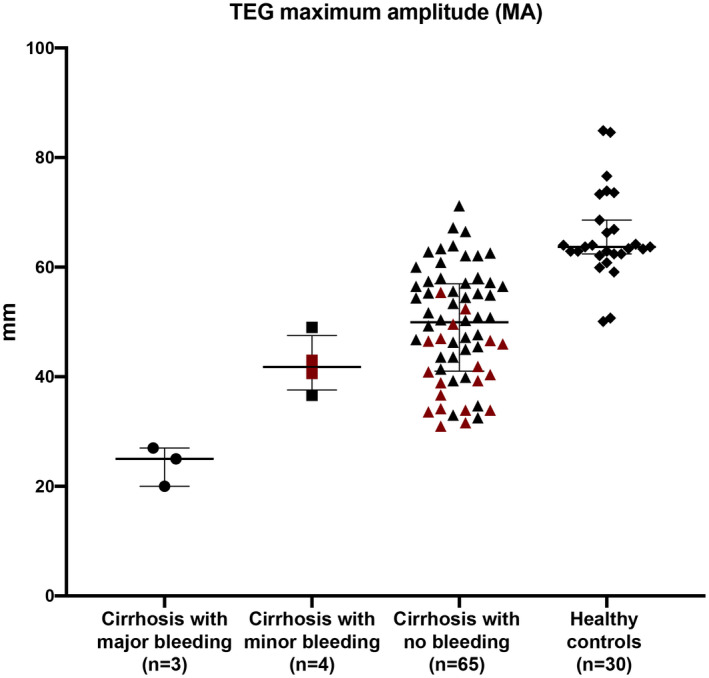
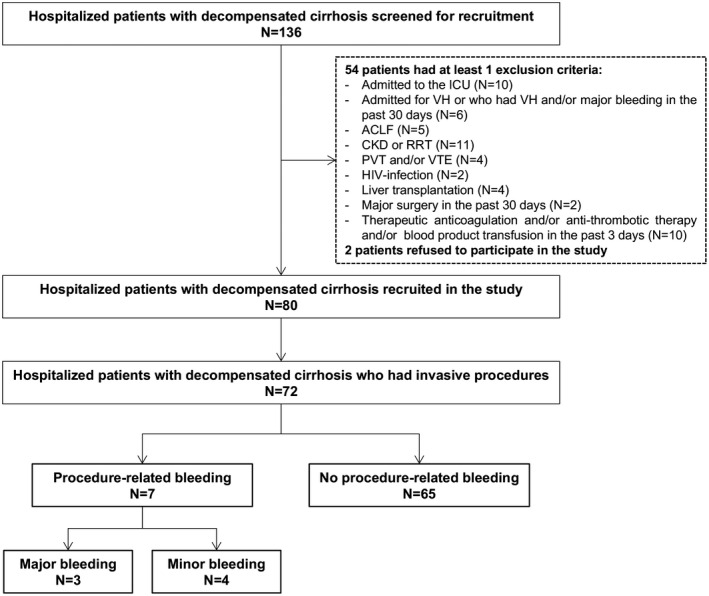
In patients with decompensated cirrhosis, procedure-related bleeding is a potentially lethal complication. Routine coagulation tests such as international normalized ratio and platelet count do not predict bleeding risk. We investigated whether thromboelastography (TEG) can identify patients with cirrhosis who are at risk of procedure-related bleeding. As a part of a prospective study on hemostasis in decompensated cirrhosis, patients had TEG performed on admission and were followed prospectively during hospitalization for the development of procedure-related bleeding. Eighty patients with cirrhosis were included. Among the 72 who had procedures performed, 7 had procedure-related bleeding, which was major in three cases (two following paracentesis and one following thoracentesis). Conventional coagulation tests were comparable between bleeding and nonbleeding patients, whereas TEG parameters of k-time (4.5 minutes vs. 2.2 minutes; = 0.02), α-angle (34° vs. 59°; = 0.003), and maximum amplitude (37 mm vs. 50 mm; = 0.004) were significantly different (all indicative of hypocoagulability). TEG maximum amplitude (MA), a marker of overall clot stability, accurately discriminated between patients who had major, life-threatening bleeding (all with MA < 30 mm) and those who had mild or no bleeding (all with MA > 30 mm), whereas a platelet count < 50 × 10/L could not discriminate between bleeding (minor or major) and nonbleeding patients. : In a prospective cohort of hospitalized patients with decompensated cirrhosis, TEG parameters associated with hypocoagulability appeared to predict procedure-related bleeding, particularly a TEG MA < 30 mm. If results are validated in a larger cohort, this could be a threshold to identify patients with decompensated cirrhosis at higher risk for procedure-related bleeding, in whom to consider preprocedural prophylaxis.
在失代偿期肝硬化患者中,与操作相关的出血是一种潜在致命的并发症。常规凝血检测(如国际标准化比值和血小板计数)不能预测出血风险。我们研究了血栓弹力图(TEG)是否可以识别有与操作相关出血风险的肝硬化患者。作为失代偿期肝硬化止血的前瞻性研究的一部分,患者在入院时进行 TEG 检查,并在住院期间前瞻性地观察与操作相关出血的发生情况。共纳入 80 例肝硬化患者。在进行了操作的 72 例患者中,有 7 例发生了与操作相关的出血,其中 3 例(2 例在进行腹腔穿刺术和 1 例在进行胸腔穿刺术时)为大出血。出血组和非出血组患者的常规凝血检测结果相似,而 TEG 参数 k-时间(4.5 分钟比 2.2 分钟; = 0.02)、α 角(34°比 59°; = 0.003)和最大振幅(37 毫米比 50 毫米; = 0.004)差异有统计学意义(均提示存在低凝状态)。TEG 最大振幅(MA),一种整体血凝块稳定性的标志物,能够准确区分发生大出血(所有 MA 值均<30 毫米)和仅有轻度出血或无出血(所有 MA 值均>30 毫米)的患者,而血小板计数<50×10/L 不能区分有出血(轻度或重度)和无出血的患者。在一项前瞻性住院失代偿期肝硬化患者队列研究中,与低凝状态相关的 TEG 参数似乎可以预测与操作相关的出血,尤其是 TEG MA<30 毫米。如果在更大的队列中得到验证,这可能是一个确定失代偿期肝硬化患者与操作相关出血风险更高的阈值,在此类患者中考虑进行术前预防。